A glimpse into the future of particle therapy
Particle therapy is an incredibly powerful cancer treatment. But it is also an incredibly expensive option that relies on massive, bulky accelerator systems. As such, in 2025 there were only 137 proton and carbon-ion therapy facilities in operation worldwide. So how can more people benefit?
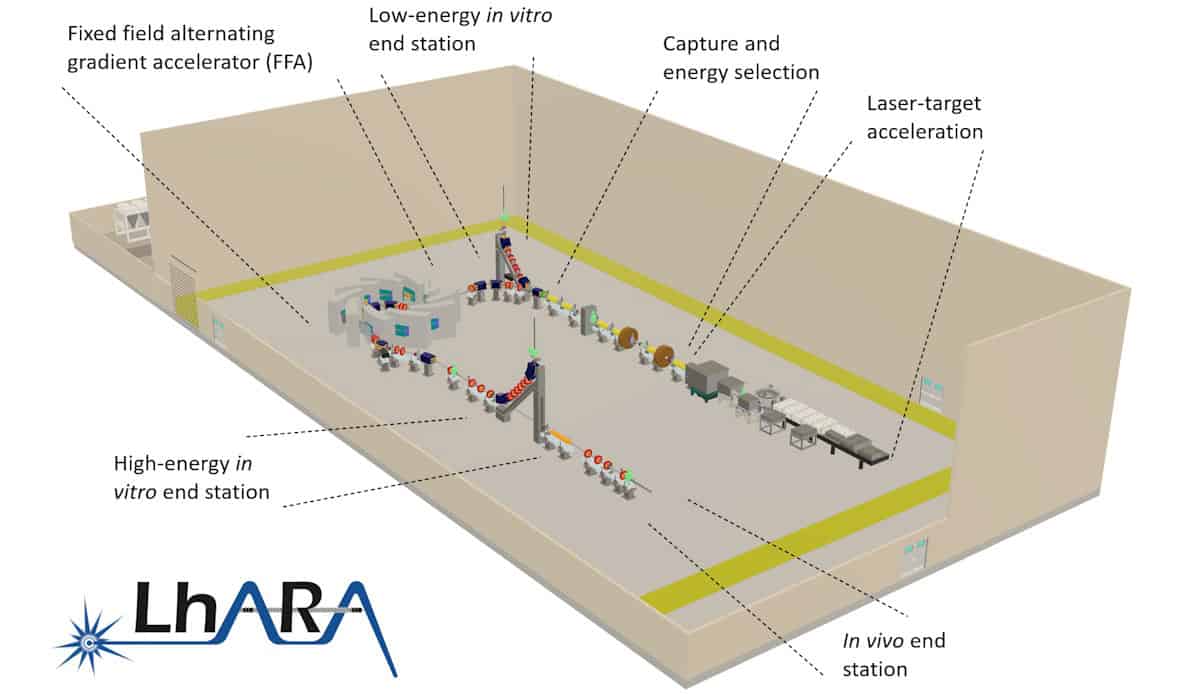
Hoping to resolve this challenge, the LhARA collaboration is investigating a new take on particle therapy delivery: a laser-hybrid accelerator for radiobiological applications. The idea is to use laser-driven proton and ion beams to create a compact, high-throughput treatment facility to advance our understanding of cancer and its response to radiation (see: “A novel hybrid design”).
Last month, in the first of a series of CP4CT workshops, experts in the field came together at Imperial College London to discuss the potential advantages of laser-driven charged particles. The workshop aimed to examine the current status of particle therapy technology, assess how the unique properties of laser-driven beams could revolutionize particle therapy, and identify the key research needed to develop personalized cancer therapy with laser-driven ions.
“We want to lay the foundation for the transformation of ion beam therapy,” said Kenneth Long (Imperial College London/STFC), who co-organized the event together with Richard Amos (University College London). “We are aiming to engage with the communities that we will target when the technology is mature.”
A novel hybrid design
LhARA uses a high-power, fast-pulsed laser to create high-flux proton and ion beams with arbitrary spatial and time structures, such as bunches as short as 10 to 40 ns. The beams are captured and focused by a novel electron-plasma lens, and then accelerated using a fixed-field alternating gradient accelerator, to energies of 15–127 MeV for protons and 5–34 MeV/u for ion beams.
The LhARA team recently completed its conceptual design report for the proposed new accelerator facility and is now running radiobiology programmes to prove the feasibility of laser-driven hybrid acceleration, for both radiation biology and clinical studies.
Particle therapy today
The day’s first speaker, Alejandro Mazal (Centro de Protonterapia Quirónsalud) pointed out that despite huge clinical potential, only about 400,000 patients have been treated with proton therapy to date (and 65,000 with carbon ions), with a typical saturation of about 250 patients per year per treatment room. To increase this throughput, factors such as image guidance, adaptive tools, uptime and modularity for upgrades could prove vital.
Mazal cited some development priorities to address, including cost control, vendor robustness, system reliability and throughput optimization. It’s also vital to consider biological modulation techniques, integration into hospitals and generation of clinical evidence. “We used to say that randomized trials are not ethical with particle therapy but this is not always true, evidence must guide expansion,” he said.
Mazal emphasized that technology itself is not the endpoint, but that specifications must be driven by clinical benefit. “The goal is to be transformative, but only when we can measure a clinical value,” he explained.
Sandro Rossi (CNAO) then presented an update on the latest developments at the National Centre of Oncological Hadronotherapy (CNAO) in Italy. Since starting clinical treatments in 2011, the facility has now treated over 6000 patients – roughly half with protons and half with carbon ions. He noted that for some of the most challenging tumours, CNAO’s particle therapy delivered considerably better local tumour control than achieved by conventional X-ray treatments.
CNAO is also a research facility, currently hosting 17 funded research projects and seven active clinical trials. Looking forward, an expansion project will see the centre commission an additional proton therapy gantry, introduce boron neutron capture therapy (BNCT) and install an upright positioning system (from Leo Cancer Care) in one of the treatment rooms.
The killer biological questions
In parallel with the development of laser-based accelerators, researchers are investigating various radiobiological modulation strategies that could enhance the impact of particle therapy. The workshop examined three such options: proton minibeams, FLASH irradiation and combination with immunotherapies.
Minibeam therapy uses an array of submillimetre-sized radiation beams to deliver a pattern of alternating high-dose peaks and low-dose valleys. This spatially fractionated dose greatly reduces treatment toxicity while providing excellent tumour control, as demonstrated in extensive preclinical experiments.
The first patient treatments (using X-ray minibeams) took place in 2024, and clinical investigations on proton minibeams are just starting, explained Yolanda Prezado (CiMUS). Recent studies revealed that minibeams induce a favourable immune response, with high T cell infiltration, vascular renormalization and reduced hypoxia dependence. Further evaluation is essential to explore the underlying radiobiological mechanisms, but Prezado noted that existing accelerators are limited in their ability to modulate treatment beams.
“It would be really interesting to have a system where we can flexibly vary all of the parameters to understand all of these techniques; LhARA could be a very interesting facility for this,” she suggested.
As for the second option, FLASH therapy, this is an emerging treatment approach in which radiation delivery at ultrahigh dose rates reduces normal tissue damage while effectively killing cancer cells. But how the FLASH effect works, and how to optimize this approach, remain key questions.
Joao Seco (DKFZ) presented a novel interpretation of FLASH, focusing on radiation chemistry and emphasizing the role of H2O2 generation in the FLASH process. Production of H2O2, a key molecule in cell damage, depends on the activity of a particular enzyme called superoxide dismutase 1 (SOD1). Seco hypothesized that inhibiting SOD1 could control H2O2 production and thus control cellular damage, effectively mimicking the FLASH effect.
“Forget radiation biology, we are missing a key component: redox chemistry,” he said. “If we know the redox chemistry, we can predict the response before we give radiotherapy.”
Marco Durante (GSI) suggested that the most urgent challenge for radiotherapy may be to combine it with immunotherapy, noting that charged particle beams offer both physical and biological advantages to achieve this. Citing various trials of combined immunotherapy and X-ray-based radiotherapy for cancer treatment, he showed some impressive examples of the benefit of the combination, but also cases with negative results.
“The question to understand is why doesn’t it always work,” he explained, suggesting that this may be due to the timing and sequencing of the two therapies, the fractionation scheme or biological factors. But perhaps a more promising approach would be to combine immunotherapy with particle therapy, he said, sharing examples where immunotherapy plus carbon-ions had better clinical outcomes than combinations with X-ray radiotherapy.
This superior outcome may arise from the various biological advantages of high-LET irradiation. Alongside, the lower integral dose from particle therapy compared with X-rays results in less lymphopenia (a low level of white blood cells), which is indicative of improved prognosis.
“Pre-clinical studies are essential to address timing and sequencing,” he concluded. “We also need more clinical trials to determine the impact of physical and biological properties of charged particles in radioimmunotherapy.”
Democratizing access
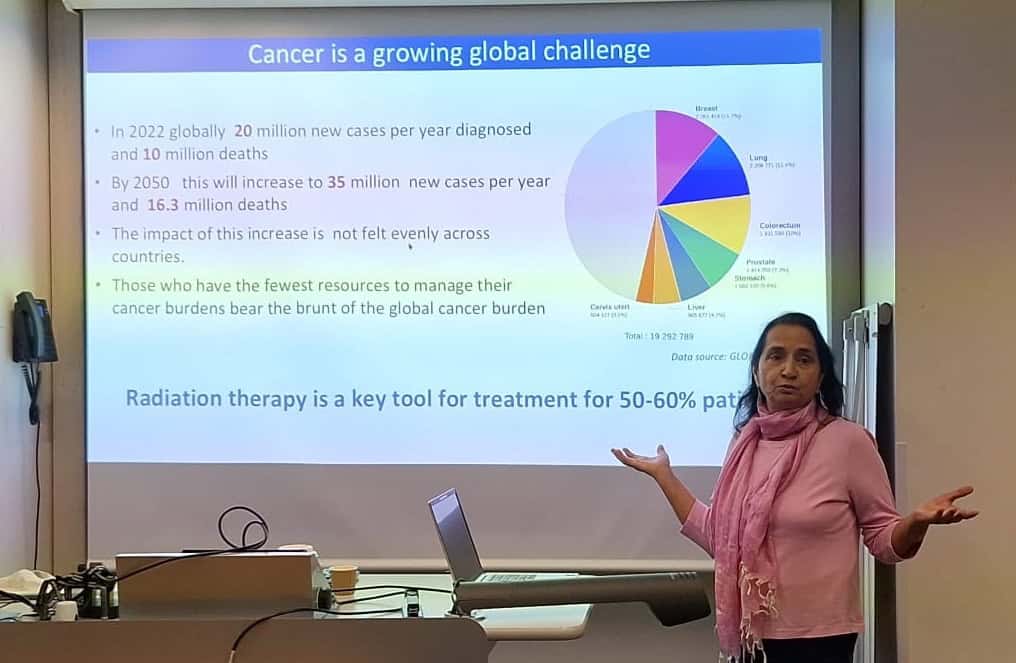
Manjit Dosanjh (University of Oxford) discussed the continuing need to increase global access to radiotherapy, noting that while radiotherapy is a key tool for over 50% of cancer patients, not all countries have access to sufficient treatment systems, nor to the expert personnel needed to run them.
Across Africa, for instance, there is just one linac per 3.5 million people, in stark contrast to the one per 86, 000 people in the US. Many European countries also lack sufficient quality or quantity of radiotherapy facilities – a disparity that’s mirrored in terms of access to CT scanners, oncologists and medical physicists, which must be addressed in tandem. “If we could improve imaging, treatments and care quality, we could prevent 9.6 million deaths per year worldwide,” Dosanjh said.
She described some initiatives designed to encourage collaboration and increase access, including ENLIGHT, the European Network for Light Ion Hadron Therapy. Launched in 2002 at CERN, ENLIGHT brings together clinicians, physicists, biologists and engineers working within particle therapy to develop new technologies and provide training, education and access to beams to move the field forward.
More recently, the STELLA (smart technologies to extend lives with linear accelerators) project was established to create a cost-effective, robust radiotherapy linac with lower staff requirements and maximal uptime. A global collaboration, STELLA aims to expand access to high-quality cancer treatment for all patients via innovative transformation of the treatment system, as well as providing training, education and mentoring.
Dosanjh also introduced SAPPHIRE, a UK-led initiative that partners with institutions in Ghana and South Africa to strengthen radiotherapy services across Africa. She stressed that improving access to radiotherapy is a big challenge that can only be achieved by building really good collaborations. “Collaboration is the invisible force that makes the impossible possible,” she said.
Konrad Nesteruk (Harvard) continued the theme of democratizing particle therapy, noting that advancement of beam technologies calls for innovations in space (the facility size), time (both irradiation and total treatment time) and dose (via techniques such as FLASH, proton arc and minibeams). All of these factors interact to create a multidimensional optimization problem, he explained.
The final speaker in this session, Rock Mackie (University of Wisconsin) examined how to translate innovative radiotherapy technology into clinical practice. Academia is the source of breakthrough ideas, he said, but most R&D is funded and refined by companies. And forming a company involves a series of key tasks: identifying an important problem; developing a technical solution; patenting it; customer testing; and procuring investment. If this final stage doesn’t happen, Mackie remarked, it wasn’t an important enough problem.
In particle therapy, the main problems are size and cost limiting patient access, a lack of effective imaging solutions and the fact that the gain in therapeutic ratio does not compensate for increased costs. Aiming to solve these problems, Mackie co-founded Leo Cancer Care in 2018 to commercialize an upright patient positioning system and CT scanner. This approach enables a proton therapy machine to fit into a photon vault, as well as easing patient positioning, thus reducing installation costs while simultaneously increasing throughput.
Mackie applied this startup scenario to LhARA. Here, the problem to solve is achieving high-energy, multi-ion, high-intensity beams for radiotherapy, FLASH, spatial fractionation and proton imaging. The solution is the development of a low-cost particle accelerator that meets all of these needs and fits in a single-storey vault. He also emphasized the importance of consulting with as many potential customers as time permits before defining specifications.
“The most important problem is finding a big enough problem to solve,” he concluded. “It will find a market if the product is less costly, works better and is easier to use.”
Development roadmap
Alexander Gerbershagen (PARTREC) told delegates about PARTREC, the particle therapy research centre at the University Medical Center Groningen. The facility’s superconducting accelerator, AGOR, provides protons with energies up to 190 MeV, as well as ion beams of all elements up to xenon. Ongoing projects at PARTREC include: developing glioblastoma treatments using boron proton capture therapy (NuCapCure); production of terbium isotopes for theranostics; image-guided pharmacotherapy using photon-activated drugs; and real-time in vivo verification of proton therapy dose.
The day closed with a look at the potential of LhARA as an international research facility. Kenneth Long emphasized the importance of investigating how ionizing radiation interacts with tissue, in vivo and in vitro, while considering all of the factors that may impact outcome. This includes time and space domains, different ion species and energies, and combinations with chemo- and immunotherapy. “If one flexible beam facility can do all that, it’s a substantial opportunity for a step change in understanding,” he said.
Long presented some initial cell irradiations using laser-driven beams at the SCAPA research centre in Strathclyde, and noted that component optimization is also underway in Swansea. He also shared designs for the envisaged research facility, with various in vivo and in vitro end-stations and robotic automation to move experiments around. “We have written a mission statement, now our business is to execute that programme,” he concluded.
The post A glimpse into the future of particle therapy appeared first on Physics World.