Cell-based biocomputing is a novel technique that uses cellular processes to perform computations. Such micron-scale biocomputers could overcome many of the energy, cost and technological limitations of conventional microprocessor-based computers, but the technology is still very much in its infancy. One of the key challenges is the creation of cell-based systems that can solve complex computational problems.
Now a research team from the Saha Institute of Nuclear Physics in India has used genetically modified bacteria to create a cell-based biocomputer with problem-solving capabilities. The researchers created 14 engineered bacterial cells, each of which functioned as a modular and configurable system. They demonstrated that by mixing and matching appropriate modules, the resulting multicellular system could solve nine yes/no computational decision problems and one optimization problem.
The cellular system, described in Nature Chemical Biology, can identify prime numbers, check whether a given letter is a vowel, and even determine the maximum number of pizza or pie slices obtained from a specific number of straight cuts. Here, senior author Sangram Bagh explains the study’s aims and findings.
How does cell-based computing work?
Living cells use computation to carry out biological tasks. For instance, our brain’s neurons communicate and compute to make decisions; and in the event of an external attack, our immune cells collaborate, compute and make judgements. The development of synthetic biology opens up new avenues for engineering live cells to carry out human-designed computation.
The fusion of biology and computer science has resulted in the development of living cell-based biocomputers to solve computational problems. Here, living cells are engineered to use as circuits and components to build biocomputers. Lately, researchers have been manipulating living cells to find solutions for maze and graph colouring puzzles.
Why did you employ bacteria to perform the computations?
Bacteria are single-cell organisms, 2–5 µm in size, with fast replication times (about 30 min). They can survive in many conditions and require minimum energy, thus they provide an ideal chassis for building micron-scale computer technology. We chose to use Escherichia coli, as it has been studied in detail and is easy to manipulate, making it a logical choice to build a biocomputer.
How did you engineer the bacteria to solve problems?
We built synthetic gene regulatory networks in bacteria in such a way that each bacterium worked as an artificial neuro-synapse. In this way, 14 genetically engineered bacteria were created, each acting like an artificial neuron, which we named “bactoneurons”. When these bactoneurons are mixed in a liquid culture in a test tube, they create an artificial neural network that can solve computational problems. The “LEGO-like” system incorporates 14 engineered cells (the “LEGO blocks”) that you can mix and match to build one of 12 specific problem solvers on demand.
How do the bacteria report their answers?
We pose problems to the bacteria in a chemical space using a binary system. The bacteria were questioned by adding (“one”) or not adding (“zero”) four specific chemicals. The bacterial artificial neural network analysed the data and responded by producing different fluorescent proteins. For example, when we asked if three is a prime number, in response to this question, the bacteria glowed green to print “yes”. Similarly, when we asked if four was a prime number, the bacteria glowed red and said “no”.
How could such a biocomputer be used in real-world applications?
Bacteria are tiny organisms, about one-twentieth the diameter of a human hair. It is not possible to make a silicon computer so small. Making such a small computer with bacteria will open a new horizon in microscale computer technology. Its use will extend from new medical technology and material technology to space technology.
For example, one may imagine a set of engineered bacteria or other cells within the human body taking decisions and acting upon a particular disease state, based on multiple biochemical and physiological cues.
Scientists have proposed using synthetically engineered organisms to help in situ resource utilization to build a human research base on Mars. However, it may not be possible to instruct each of the organisms remotely to perform a specific task based on local conditions. Now, one can imagine the tiny engineered organisms working as a biocomputer, interacting with each other, and taking autonomous decisions on action without any human intervention.
The importance of this work in basic science is also immense. We know that recognizing prime numbers or vowels can only be done by humans or computers – but now genetically engineered bacteria are doing the same. Such observations raise new questions about the meaning of “intelligence” and offer some insight on the biochemical nature and the origin of intelligence.
What are you planning to do next?
We would like to build more complex biocomputers to perform more complex computation tasks with multitasking capability. The ultimate goal is to build artificially intelligent bacteria.
GenesisCare is the largest private radiation oncology provider in Australia, operating across five states and treating around 30,000 cancer patients each year. At the heart of this organization, ensuring the safety and efficiency of all patient radiotherapy treatments, lies a single server running LAP’s RadCalc quality assurance (QA) software.
RadCalc is a 100% software-based platform designed to streamline daily patient QA. The latest release, version 7.3.2, incorporates advanced 3D algorithms for secondary verification of radiotherapy plans, EPID-based pre-treatment QA and in vivo dosimetry, as well as automated 3D calculation based on treatment log files.
For GenesisCare, RadCalc provides independent secondary verification for 100 to 130 new plans each day, from more than 43 radiation oncology facilities across the country. The use of a single QA platform for all satellite centres helps to ensure that every patient receives the same high standard of care. “With everyone using the same software, we’ve got a single work instruction and we’re all doing things the same way,” says Leon Dunn, chief medical physicist at GenesisCare in Victoria.
“While the individual states operate as individual business units, the physics team operates as one, and the planners operate as one team as well,” adds Peter Mc Loone, GenesisCare’s head of physics for Australia. “We are like one team nationally, so we try to do things the same way. Obviously, it makes sense to make sure everyone’s checking the plans in the same way as well.”
User approved
GenesisCare implemented RadCalc more than 10 years ago, selected in part due to the platform’s impressive reputation amongst its users in Australia. “At that time, RadCalc was well established in radiotherapy and widely used,” explains Dunn. “It didn’t have all the features that it has now, but its basic features met the requirements we needed and it had a pretty solid user base.”
Today, GenesisCare’s physicists employ RadCalc for plan verification of all types of treatment across a wide range of radiotherapy platforms – including Varian and Elekta linacs, Gamma Knife and the Unity MR-linac, as well as superficial treatments and high dose-rate brachytherapy. They also use RadCalc’s plan comparison tool to check that the output from the treatment planning system matches what was imported to the MOSAIQ electronic medical record system.
“Before we had the plan comparison feature, our radiation therapists had to manually check control points in the plan against what was on the machine,” says Mc Loone. “RadCalc checks a wide range of values within the plan. It’s a very quick check that has saved us a lot of time, but also increased the safety aspect. We have certainly picked up errors through its use.”
Keeping treatments safe
The new feature that’s helping to make a big difference, however, is GenesisCare’s recent implementation of RadCalc’s 3D independent recalculation tool. Dunn explains that RadCalc previously performed a 2D comparison between the dose to a single point in the treatment planning system and the calculated dose to that point.
The new module, on the other hand, employs RadCalc’s collapsed-cone convolution algorithm to reconstruct 3D dose on the patient’s entire CT data set. Enabled by the introduction of graphics processing units, the algorithm performs a completely independent 3D recalculation of the treatment plan on the patient’s data. “We’ve gone from a single point to tens of thousands of points,” notes Dunn.
Importantly, this 3D recalculation can discover any errors within a treatment plan before it gets to the point at which it needs to be measured. “Our priority is for every patient to have that second check done, thereby catching anything that is wrong with the treatment plan, hopefully before it is seen by the doctor. So we can fix things before they could become an issue,” Dunn says, pointing out that in the first couple of months of using this tool, it highlighted potentially suboptimal treatment plans to be improved.
Peter Mc Loone: “It’s a very quick check that has saved us a lot of time, but also increased the safety aspect.” (Courtesy: GenesisCare)
In contrast, previous measurement-based checks had to be performed at the end of the entire planning process, after everyone had approved the plan and it had been exported to the treatment system. “Finding an error at that point puts a lot of pressure on the team to redo the plan and have everything reapproved,” Mc Loone explains. “By removing that stress and allowing checks to happen earlier in the piece, it makes the overall process safer and more efficient.”
Dunn notes that if the second check shows a problem with the plan, the plan can still be sent for measurements if needed, to confirm the RadCalc findings.
Increasing efficiency
As well as improving safety, the ability to detect errors early on in the planning process speeds up the entire treatment pathway. Operational efficiency is additionally helped by RadCalc’s high level of automation.
Once a treatment plan is created, the planning staff need to export it to RadCalc, with a single click. RadCalc then takes care of everything else, importing the entire data set, sending it to the server for recalculation and then presenting the results. “We don’t have to touch any of the processes until we get the quality checklist out, and that’s a real game changer for us,” says Dunn.
“We have one RadCalc system, that can handle five different states and several different treatment planning systems [Varian’s Eclipse and Elekta’s Monaco and GammaPlan],” notes Mc Loone. “We can have 130 different plans coming in, and RadCalc will filter them correctly and apply the right beam models using that automation that LAP has built in.”
Because RadCalc performs 100% software-based checks, it doesn’t require access to the treatment machine to run the QA (which usually means waiting until the day’s clinical session has finished). “We’re no longer waiting around to perform measurements on the treatment machine,” Dunn explains. “It’s all happening while the patients are being treated during the normal course of the day. That automation process is an important time saver for us.”
This shift from measurement- to software-based QA also has a huge impact on the radiation therapists. As they were already using the machines to treat patients, the therapists were tasked with delivering most of the QA cases – at the end of the day or in between treatment sessions – and informing the physicists of any failures.
“Since we’ve introduced RadCalc, they essentially get all that time back and can focus on doing what they do best, treating patients and making sure it’s all done safely,” says Dunn. “Taking that burden away from them is a great additional bonus.”
Looking to the future, GenesisCare next plans to implement RadCalc’s log file analysis feature, which will enable the team to monitor and verify the performance of the radiotherapy machines. Essentially, the log files generated after each treatment are brought back into RadCalc, which then verifies that what the machine delivered matched the original treatment plan.
“Because we have so many plans going through, delivered by many different accelerators, we can start to build a picture of machine performance,” says Dunn. “In the future, I personally want to look at the data that we collect through RadCalc. Because everything’s coming through that one system, we’ve got a real opportunity to examine safety and quality at a system level, from treatment planning system through to patient treatment.”
Osteosarcoma, the most common type of bone tumour, is a highly malignant cancer that mainly affects children and young adults. Patients are typically treated with an aggressive combination of resection and chemotherapy, but survival rates have not improved significantly since the 1970s. With alternative therapies urgently needed, a research team at Aston University has developed a gallium-doped bioactive glass that selectively kills over 99% of bone cancer cells.
The main objective of osteosarcoma treatment is to destroy the tumour and prevent recurrence. But over half of long-term survivors are left with bone mass deficits that can lead to fractures, making bone restoration another important goal. Bioactive glasses are already used to repair and regenerate bone – they bond with bone tissue and induce bone formation by releasing ions such as calcium, phosphorus and silicon. But they can also be designed to release therapeutic ions.
Team leader Richard Martin and colleagues propose that bioactive glasses doped with gallium ions could address both tasks – helping to prevent cancer recurrence and lowering the risk of fracture. They designed a novel biomaterial that provides targeted drug delivery to the tumour site, while also introducing a regenerative scaffold to stimulate the new bone growth.
“Gallium is a toxic ion that has been widely studied and is known to be effective for cancer therapy. Cancer cells tend to be more metabolically active and therefore uptake more nutrients and minerals to grow – and this includes the toxic gallium ions,” Martin explains. “Gallium is also known to inhibit bone resorption, which is important as bone cancer patients tend to have lower bone density and are more prone to fractures.”
Glass design
Starting with a silicate-based bioactive glass, the researchers fabricated six glasses doped with between 0 and 5 mol% of gallium oxide (Ga2O3). They then ground the glasses into powders with a particle size between 40 and 63 µm.
Martin notes that gallium is a good choice for incorporating into the glass, as it is effective in a variety of simple molecular forms. “Complex organic molecules would not survive the high processing temperatures required to make bioactive glasses, whereas gallium oxide can be incorporated relatively easily,” he says.
To test the cytotoxic effects of the bioactive glasses on cancer cells, the team created “conditioned media”, by incubating the gallium-doped glass particles in cell culture media at concentrations of 10 or 20 mg/mL. After 24 h, the particles were filtered out to leave various levels of gallium ions in the media.
The researchers then exposed osteosarcoma cells, as well as normal osteoblasts as controls, to conditioned media from the six gallium-doped powders. Cell viability assays revealed significant cytotoxicity in cancer cells exposed to the conditioned media, with a reduction in cell viability correlating with gallium concentration.
After 10 days, cancer cells exposed to media conditioned with 10 mg/mL of 4 and 5% gallium-doped glass showed decreased cell viability, to roughly 60% and less than 10%, respectively. The 20 mg/mL of 4% and 5% gallium-doped glass were the most toxic to the cancer cells, causing 60% and more than 99% cell death, respectively, after 10 days.
Exposure to gallium-free bioglass did not significantly impact cell viability – confirming that the toxicity is due to gallium and not the other components of the glass (calcium, sodium, phosphorus and silicate ions).
While the glasses preferentially killed osteosarcoma cells compared with normal osteoblasts, some cytotoxic effects were also seen in the control cells. Martin believes that this slight toxicity to normal healthy cells is within safe limits, noting that the localized nature of the treatment should significantly reduce side effects compared with orally administered gallium.
“Further experiments are needed to confirm the safety of these materials,” he says, “but our initial studies show that these gallium-doped bioactive glasses are not toxic in vivo and have no effects on major organs such as the liver or kidneys.”
The researchers also performed live/dead assays on the osteosarcoma and control cells. The results confirmed the highly cytotoxic effect of gallium-doped bioactive glass on the cancer cells with relatively minor toxicity towards normal cells. They also found that exposure to the gallium-doped glass significantly reduced cancer cell proliferation and migration.
Bone regeneration
To test whether the bioactive glasses could also help to heal bone, the team exposed glass samples to simulated body fluid for seven days. Under these physiological conditions, the glasses gradually released calcium and phosphorous ions.
FTIR and energy dispersive X-ray spectroscopy revealed that these ions precipitated onto the glass surface to form an amorphous calcium phosphate/hydroxyapatite layer – indicating the initial stages of bone regeneration. For clinical use, the glass particles could be mixed into a paste and injected into the void created during tumour surgery.
“This bioactivity will help generate new bone formation and prevent bone mass deficits and potential future fractures,” Martin and colleagues conclude. “The results when combined strongly suggest that gallium-doped bioactive glasses have great potential for osteosarcoma-related bone grafting applications.”
Next, the team plans to test the materials on a wide range of bone cancers to ensure the treatment is effective against different cancer types, as well as optimizing the dosage and delivery before undertaking preclinical tests.
A magnetically controlled prosthetic hand, tested for the first time in a participant with an amputated lower arm, provided fine control of hand motion and enabled the user to perform everyday actions and grasp fragile objects. The robotic prosthetic, developed by a team at Scuola Superiore Sant’Anna in Pisa, uses tiny implanted magnets to predict and carry out intended movements.
Losing a hand can severely affect a person’s ability to perform everyday work and social activities, and many researchers are investigating ways to restore lost motor function via prosthetics. Most available or proposed strategies rely on deciphering electrical signals from residual nerves and muscles to control bionic limbs. But this myoelectric approach cannot reproduce the dexterous movements of a human hand.
Instead, Christian Cipriani and colleagues developed an alternative technique that exploits the physical displacement of skeletal muscles to decode the user’s motor intentions. The new myokinetic interface uses permanent magnets implanted into the residual muscles of the user’s amputated arm to accurately control finger movements of a robotic hand.
“Standard myoelectric prostheses collect non-selective signals from the muscle surface and, due to that low selectivity, typically support only two movements,” explains first author Marta Gherardini. “In contrast, myokinetic control enables simultaneous and selective targeting of multiple muscles, significantly increasing the number of control sources and, consequently, the number of recognizable movements.”
First-in-human test
The first patient to test the new prosthesis was a 34-year-old named Daniel, who had recently lost his left hand and had started to use a myoelectric prosthesis. The team selected him as a suitable candidate because his amputation was recent and blunt, he could still feel the lost hand and the residual muscles in his arm moved in response to his intentions.
For the study, the team implanted six cylindrical (2 mm radius and height) neodymium magnets coated with a biocompatible shell into three muscles in Daniel’s residual forearm. In a minimally invasive procedure, the surgeon used plastic instruments to manipulate the magnets into the tip of the target muscles and align their magnetic fields, verifying their placement using ultrasound.
Daniel also wore a customized carbon fibre prosthetic arm containing all of the electronics needed to track the magnets’ locations in space. When he activates the residual muscles in his arm, the implanted magnets move in response to the muscle contractions. A grid of 140 magnetic field sensors in the prosthesis detect the position and orientation of these magnets and transmit the data to an embedded computing unit. Finally, a pattern recognition algorithm translates the movements into control signals for a Mia-Hand robotic hand.
Gherardini notes that the pattern recognition algorithm rapidly learnt to control the hand based on Daniel’s intended movements. “Training the algorithm took a few minutes, and it was immediately able to correctly recognize the movements,” she says.
In addition to the controlled hand motion arising from intended grasping, the team found that elbow movement activated other forearm muscles. Tissue near the elbow was also compressed by the prosthetic socket during elbow flexion, which caused unintended movement of nearby magnets. “We addressed this issue by estimating the elbow movement through the displacement of these magnets, and adjusting the position of the other magnets accordingly,” says Gherardini.
During the six-week study, the team performed a series of functional tests commonly used to assess the dexterity of upper limb prostheses. Daniel successfully completed these tests, with comparable performance to that achieved using a traditional myoelectric prosthetic (in tests performed before the implantation surgery).
Importantly, he was able to control finger movements well enough to perform a wide range of everyday activities – such as unscrewing a water bottle cap, cutting with a knife, closing a zip, tying shoelaces and removing pills from a blister pack. He could also control the grasp force to manipulate fragile objects such as an egg and a plastic cup.
The researchers report that the myokinetic interface worked even better than they expected, with the results highlighting its potential to restore natural motor control in people who have lost limbs. “This system allowed me to recover lost sensations and emotions: it feels like I’m moving my own hand,” says Daniel in a press statement.
At the end of the six weeks, the team removed the magnets. Asides for low-grade inflammation around one magnet that had lost its protective shell, all of the surrounding tissue was healthy. “We are currently working towards a long-term solution by developing a magnet coating that ensures long-term biocompatibility, allowing users to eventually use this system at home,” Gherardini tells Physics World.
She adds that the team is planning to perform another test of the myokinetic prosthesis within the next two years.
Enhancing the dose Dose distributions for a pancreatic ductal carcinoma case and a pancreatic adenocarcinoma case, for GNP-enhanced 2.5 MV plans (left) and 6 MV beams without GNPs (right). (Courtesy: Phys. Med. Biol. 10.1088/1361-6560/ad68be)
The primary goal of radiotherapy is to effectively destroy the tumour while minimizing side effects to nearby normal tissues. Focusing on the challenging case of pancreatic cancer, a research team headed up at Toronto Metropolitan University in Canada has demonstrated that gold nanoparticles (GNPs) show potential to optimize this fine balance between tumour control probability (TCP) and normal tissue complication probability (NTCP).
GNPs are under scrutiny as candidates for improving the effectiveness of radiation therapy by enhancing dose deposition within the tumour. The dose enhancement observed when irradiating GNP-infused tumour tissue is mainly due to the Auger effect, in which secondary electrons generated within the nanoparticles can damage cancer cells.
“Nanoparticles like GNPs could be delivered to the tumour using targeting agents such as [the cancer drug] cetuximab, which can specifically bind to the epidermal growth factor receptor expressed on pancreatic cancer cells, ensuring a high concentration of GNPs in the tumour site,” says first author Navid Khaledi, now at CancerCare Manitoba.
This increased localized energy deposition should improve tumour control; but it’s also crucial to consider possible toxicity to normal tissues due to the presence of GNPs. To investigate this further, Khaledi and colleagues simulated treatment plans for five pancreatic cancer cases, using CT images from the Cancer Imaging Archive database.
Plan comparison
For each case, the team compared plans generated using a 2.5 MV photon beam in the presence of GNPs with conventional 6 MV plans. “We chose a 2.5 MV beam due to the enhanced photoelectric effect at this energy, which increases the interaction probability between the beam and the GNPs,” Khaledi explains.
The researchers created the treatment plans using the MATLAB-based planning program matRad. They first determined the dose enhancement conferred by 50-nm diameter GNPs by calculating the relative biological effectiveness (RBE, the ratio of dose without to dose with GNPs for equal biological effects) using custom MATLAB codes. The average RBE for the 2.5 MV beam, using α and β radiosensitivity values for pancreatic tumour, was 1.19. They then applied RBE values to each tumour voxel to calculate dose distributions and TCP and NTCP values.
The team considered four treatment scenarios, based on a prescribed dose of 40 Gy in five fractions: 2.5 MV plus GNPs, designed to increase TCP (using the prescribed dose, but delivering an RBE-weighted dose of 40 Gy x 1.19); 2.5 MV plus GNPs, designed to reduce NTCP (lowering the prescribed dose to deliver an RBE-weighted dose of 40 Gy); 6 MV using the prescribed dose; and 6 MV with the prescribed dose increased to 47.6 Gy (40 Gy x 1.19).
The analysis showed that the presence of GNPs significantly increased TCP values, from around 59% for the standard 6 MV plans to 93.5% for the 2.5 MV plus GNPs (increased TCP) plans. Importantly, the GNPs helped to maintain low NTCP values of below 1%, minimizing the risk of complications in normal tissues. Using a conventional 6 MV beam with an increased dose also resulted in high TCP values, but at the cost of raising NTCP to 27.8% in some cases.
Minimizing risks
The team next assessed the dose to the duodenum, the main dose-limiting organ for pancreatic radiotherapy. The mean dose to the duodenum was highest for the increased-dose 6 MV photon beam, and lowest for the 2.5 MV plus GNPs plans. Similarly, D2%, the maximum dose received by 2% of the volume, was highest with the increased-dose 6 MV beam, and lowest with 2.5 MV plus GNPs.
It’s equally important to consider dose to the liver and kidney, as these organs may also uptake GNPs. The analysis revealed relatively low doses to the liver and left kidney for all treatment options, with mean dose and D2% generally below clinically significant thresholds. The highest mean doses to the liver and left kidney for 2.5 MV plus GNPs were 3.3 and 7.7 Gy, respectively, compared with 2.3 and 8 Gy for standard 6 MV photons.
The researchers conclude that the use of GNPs in radiation therapy has potential to significantly improve treatment outcomes and benefit cancer patients. Khaledi notes, however, that although GNPs have shown promise in preclinical studies and animal models, they have not yet been tested for radiotherapy enhancement in human subjects.
Next, the team plans to investigate new linac targets that could potentially enable therapeutic applications. “One limitation of the current 2.5 MV beam is its low dose rate (60 MU/min) on TrueBeam linacs, primarily due to the copper target’s heat tolerance,” Khaledi tells Physics World. “Increasing the dose rate could make the beam clinically useful, but it risks melting the copper target. Future work will evaluate the beam spectrum for different target designs and materials.”
Drowsiness plays a major role in traffic crashes, injuries and deaths, and is considered the most critical hazard in construction and mining. A wearable device that can monitor fatigue could help protect drivers, pilots and machine operators from the life-threatening dangers of fatigue.
With this aim, researchers at UC Berkeley are developing techniques to detect signs of drowsiness in the brain, using a pair of prototype earbuds to perform electroencephalography (EEG) and other physiological measurements. Describing the device in Nature Communications, the team reports successful tests on volunteers.
“Wireless earbuds are something we already wear all the time,” says senior author Rikky Muller in a press statement. “That’s what makes ear EEG such a compelling approach to wearables. It doesn’t require anything extra. I was inspired when I bought my first pair of Apple’s AirPods in 2017. I immediately thought, ‘What an amazing platform for neural recording’.”
Improved design
EEG uses multiple electrodes placed on the scalp to non-invasively monitor the brain’s electrical activity – such as the alpha waves that increase when a person is relaxed or sleepy. Researchers have also demonstrated that multi-channel EEG signals can be recorded from inside the ear canal, using in-ear sensors and electrodes.
Existing in-ear devices, however, mostly use wet electrodes (which necessitate skin-preparation and hydrogel on the electrodes), contain bulky electronics and require customized earpieces for each user. Instead, Muller and colleagues aimed to create an in-ear EEG with long-lifespan dry electrodes, wireless electronics and a generic earpiece design.
Generic design Schematic of the ear EEG (left) and the earpiece being worn by a user (right). (Courtesy: Ryan Kaveh/UC Berkeley)
The researchers developed a fabrication process based on 3D printing of a polymer earpiece body and electrodes. They then plated the electrodes with copper, nickel and gold, creating electrodes that remain stable over months of use. To ensure comfort for all users, they designed small, medium and large earpieces (with slightly different electrode sizes to maximize electrode surface area).
The final medium-sized earpiece contains four 60 mm2 in-ear electrodes, which apply outward pressure to lower the electrode–skin impedance and improve mechanical stability, plus two 3 cm2 out-ear electrodes. Signals from the earpiece are read out and transmitted to a base station by a low-power wireless neural recording platform (the WANDmini) affixed to a headband.
Drowsiness study
To assess the earbuds’ performance, the team recorded 35 h of electrophysiological data from nine volunteers. Subjects wore two earpieces and did not prepare their skin beforehand or apply hydrogel to the electrodes. As well as EEG, the device measured signals such as heart beats (using electrocardiography) and eye movements (via electrooculography), collectively known as ExG.
To induce drowsiness, subjects played a repetitive reaction time game for 40–50 min. During this task, they rated their drowsiness every 5 min on the Karolinska Sleepiness Scale (KSS). The measured ExG data, reaction times and KSS ratings were used to generate labels for classifier models. Data were labelled as “drowsy” if the user reported a KSS score of 5 or higher and their reaction time had more than doubled since the first 5 min.
To create the alert/drowsy classifier, the researchers extracted relevant temporal and spectral features in standard EEG frequency bands (delta, theta, alpha, beta and gamma). They used these data to train three low-complexity machine learning models: logistic regression, support vector machines (SVM) and random forest. They note that spectral features associated with eye movement, relaxation and drowsiness were the most important for model training.
All three classifier models achieved high accuracy, with comparable performance to state-of-the-art wet electrode systems. The best-performing model (utilizing a SVM classifier) achieved an average accuracy of 93.2% when evaluating users it had seen before and 93.3% with never-before-seen users. The logistic regression model, meanwhile, is more computationally efficient and requires significantly less memory.
The researchers conclude that the results show promise for developing next-generation wearables that can monitor brain activity in work environments and everyday scenarios. Next, they will integrate the classifiers on-chip to enable real-time brain-state classification. They also intend to miniaturize the hardware to eliminate the need for the WANDmini.
“We plan to incorporate all of the electronics into the earbud itself,” Muller tells Physics World. “We are working on earpiece integration, and new applications, including the use of earbuds during sleep.”
Alzheimer’s disease is a neurodegenerative disorder with limited treatment options. The causes of Alzheimer’s are complex and not entirely understood. It is commonly thought, however, that the build-up of amyloid-beta plaques and tangles of tau proteins in the brain leads to nerve cell death and dementia. A team at the University of Utah is investigating a new way to use radiation to reduce such deposits and potentially alleviate Alzheimer’s symptoms.
Developing a therapy for Alzheimer’s disease is a key goal for many researchers. One recent study, for example, showed evidence that reducing amyloid-beta plaques with a newly approved antibody-based drug improved cognition in patients with early-stage Alzheimer’s. Alongside, scientists are studying non-pharmacological approaches such as whole-brain, low-dose ionizing radiation, which has been shown to break up plaques in mice and exhibited a positive cognitive effect in preliminary clinical studies.
While promising, whole-brain irradiation unavoidably delivers radiation dose to healthy tissues. Instead, the University of Utah team is exploring the potential of targeted alpha therapy (TAT) to reduce amyloid plaque concentrations while minimizing damage to healthy tissue and the associated side effects.
“Our goal was to build on these studies and, as opposed to irradiating the whole brain, target the plaques specifically,” explains lead author Tara Mastren. “TAT could have potential benefits compared to the current antibody treatment, as much smaller doses are required to achieve an effect. Currently, it is hard to say if it will be better as this is new territory and studies need to be done to prove that.”
Targeted irradiation
TAT works by delivering an alpha particle-emitting radionuclide directly to a target, where it releases energy into its immediate surroundings. As alpha particles only travel a few micrometres in tissue, they deliver a highly localized dose. The approach has already proved effective for treating metastatic cancers, and the Utah team postulated that it could also be used to break bonds within amyloid-beta aggregates and facilitate plaque clearance.
To perform TAT, Mastren and colleagues synthesized a compound called BPy (a benzofuran pyridyl derivative) that targets amyloid-beta plaques. They linked BPy to the radionuclide bismuth-213 (213Bi), which has a short half-life of 46 min and decays by emitting a single alpha particle, thereby creating [213Bi]-BiBPy.
To examine whether TAT could reduce amyloid-beta concentrations, the researchers incubated [213Bi]-BiBPy with homogenates created from the brain tissue of mice genetically modified to develop amyloid plaques. After 24 h, they measured the concentration of amyloid-beta in the samples using Western blot and enzyme-linked immunosorbent assays.
Both analysis methods revealed a significant, dose-dependent reduction in amyloid-beta following incubation with [213Bi]-BiBPy, with plaque reduced to below the detection limits. Incubating the brain homogenate with free 213Bi also reduced levels of amyloid-beta, but to a significantly lesser extent. Other proteins in the homogenate were not affected, suggesting a lack of off-target damage.
The team found that a dose of 0.01488 MBq per picogram of amyloid beta was required to reduce amyloid by 50% in vitro. Mastren notes that this finding must now be investigated in vivo, as biological processes in a living brain differ from those in postmortem tissue. “However, this value gives a starting point for our in vivo studies,” she adds.
To confirm the targeted binding of [213Bi]-BiBPy, the researchers also examined 10 µm-thick brain tissue sections from the mice. They stained the sections with a fluorescent BPy probe (fluorescein-functionalized) and with thioflavin-S, an amyloid stain. Thioflavin-S revealed a dense presence of plaques, particularly in the cortex. The fluorescent BPy probe also stained plaques in the cortex, but less intensely and with more off-site binding. This finding highlights the need to investigate alternative targeting vectors to reduce white-matter binding.
The researchers conclude that TAT can significantly reduce amyloid-beta aggregates in vitro, paving the way for studies in live animals and eventually in humans. As such, they plan to start in vivo testing of TAT later this year.
“Initially, we will be looking at the biodistribution, ability to cross the blood–brain barrier, immune response to treatment and effects on plaque concentrations,” says Mastren. “If successful, we hope to follow up with testing cognitive response to treatment.”
Imaging plays a vital role in diagnosing brain disease and disorders, as well as advancing our understanding of how the human brain works. Existing brain imaging modalities, however, usually require the subject to lie flat and motionless – precluding use in people who cannot remain still or studies of the brain in motion.
To address these limitations, neuroscientists at West Virginia University have developed a wearable, motion-compatible brain positron emission tomography (PET) imager and demonstrated its use in a real-world setting. The device, described in Communications Medicine, could potentially enable previously impossible neuroimaging studies.
“We wanted to create and test a tool that could grant access to imaging the brain – including deep areas – while humans are moving around,” explains senior author Julie Brefczynski-Lewis. “We hope our device could allow the investigation of research questions related to natural upright behaviours, or the study of patients who are normally sedated due to movement issues or challenges in understanding the need to be perfectly still for a scan, which could happen with cognitive impairments or dementias.”
PET scans provide information on neuronal and functional activity by imaging the uptake of radioactive tracers in the brain. But clinical PET systems are extremely sensitive to motion and require supine (lying down) imaging and dedicated scanning rooms. There are neuroimaging techniques that can be used with patients upright and moving – such as functional near-infrared spectroscopy and high-density diffuse optical tomography – but these optical approaches only image the brain surface. Activity in deep brain structures remains unseen.
To enable upright and motion-tolerant imaging, Brefczynski-Lewis and colleagues designed the AMPET (ambulatory motion-enabling positron emission tomography), a helmet-like device that moves along with the subject’s head. The imager is made from a ring of 12 lightweight detector modules, each comprising arrays of silicon photomultipliers coupled to pixelated scintillation crystal arrays. The imager ring has a 21 cm field-of-view and a central spatial resolution of 2 mm in the tangential direction and 2.8 mm in the radial direction.
Real-world scenarios
The researchers tested the AMPET device on 11 volunteer patients who were scheduled for a clinical PET scan on the same day. The helmet was positioned the on the participant’s head such that it imaged the top of the brain, comprising the primary motor areas. Although it only weighs 3 kg, the team chose to suspend the helmet from above so that participants would not feel any weight while moving their head.
Patients received a low dose (10–20% of their total prescription) of the metabolic PET tracer 18F-FDG. “We chose a very low dose that was within the daily dose for clinical patients,” says Brefczynski-Lewis. “Some applications may require a slightly higher dose for extra sensitivity, but because the detectors are so close to the head, a full clinical-like dose would not likely be necessary.”
Immediately after tracer injection, each participant underwent AMPET imaging for 6 min while they switched between standing still and walking-in-place every 30 s. Following a 5 min transition, subjects were then scanned for another 5 min while alternating between sitting still and lifting their leg while seated. In this second imaging session, the team moved the AMPET lower around the head for five participants, to image deeper brain structures.
Meeting the goals
The team defined three goals to validate the AMPET prototype: motion artefacts of less than 2 mm; differential activation of cortical regions of interest (ROIs) related to leg movement; and differential activation to walking movements in deep brain structures.
The walking versus standing task allowed the researchers to test for any motion of the imager relative to the head. They observed an average movement-related misalignment of just 1.3 mm. Analysis of task-related activity showed the expected brain image patterns during walking, with activity in ROIs that control leg movements significantly greater than in all other imaged ROIs.
In four participants where activity was measured from deep brain structures (the fifth had incorrect helmet placement), the team observed differential activation in various deep lying structures, including the basal nuclei.
The researchers note that one volunteer had a prosthetic right leg. While performing upright walking, his brain patterns showed greater metabolic activity in the area that represented the intact leg. In contrast, no difference in activity between left and right leg ROIs was measured in the other participants.
Brefczynski-Lewis tells Physics World that patients found the AMPET reasonably comfortable and did not feel its weight on their head or neck. Certain movements, however, were slightly inhibited, especially tilting the head towards the shoulders. “Our engineer collaborators recommended a gyroscope mechanism to enable free movement in all directions,” she says.
As well as validating the prototype, the study also identified upgrades required for the AMPET and similar systems. “The great thing about a real-world study on humans was that it showed us which logistics to optimize,” explains Brefczynski-Lewis. “We are developing a system for good placement and monitoring the alignment of the imager relative to the head, as well as widening the coverage to increase sensitivity, and testing a movement task using a bolus-infusion paradigm.”
Nuclear reactors – whether operational or undergoing decommissioning – create radioactive waste. Management of this waste is a critical task and this practice has been optimized over the past few decades. Nevertheless, strategies for nuclear waste disposal employed back in the 1960s and 70s were far from ideal, and the consequences remain for today’s scientists and engineers to deal with.
In the UK, spent nuclear fuel is typically stored in ponds or water-filled silos. The water provides radiation shielding, as well as a source of cooling for the heat generated by this material. In England and Wales, the long-term disposal strategy involves ultimately transferring the waste to a deep geological disposal facility, while in Scotland, near-surface disposal is considered appropriate.
The problem, however, is that some of the legacy storage sites are many decades old and some are at risk of leaking. And when this radioactive waste leaks it can contaminate surrounding land and groundwater. The potential for radioactive contamination to get into the wet environment is an ongoing problem, particularly at legacy nuclear reactor sites.
“The strategy for waste storage 50 years ago was different to that used now. There wasn’t the same consideration for where this waste would be disposed of long term,” explains Malcolm Joyce, distinguished professor of nuclear engineering at Lancaster University. “A common assumption might have been ‘well it’s going to go in the ground at some point’ whereas actually, disposal is a necessarily rigorous, regulated and complicated programme.”
In one example, explains Joyce, radioactive waste was stored temporarily in drums and sited in near-surface spaces. “But the drums have corroded over time and they’ve started to deteriorate, putting containment at risk and requiring secondary containment protection,” he says. “Elsewhere, some of the larger ponds in which spent nuclear fuel was stored are also deteriorating and risking loss of containment.”
Problematic radioisotopes
The process of nuclear fission generates a range of radioactive products with a variety of half-lives and levels of radiotoxicity – a complex factor governed by their chemistry and radioactivity behaviours. One contaminant of particular concern is strontium-90 (Sr-90), a relatively high-yield fission product found in significant amounts in spent nuclear fuel and other radioactive waste.
Sr-90 emits relatively high-energy (0.6 MeV) beta radiation, has a relatively short half-life (about 30 years) and is water soluble, enabling it to migrate with groundwater. The major hazard, however, is its potential for uptake into biological systems. As a group 2 element similar to calcium, Sr-90 is a “bone seeker” that’s taken up by the bones and remains there, increasing the risk of leukaemia and bone cancer.
“The other challenge with strontium is that its daughter is even worse in radiotoxicity terms,” explains Joyce. Sr-90 decays into yttrium-90 (Y-90), which emits very high-energy beta radiation (2.2 MeV) that can penetrate up to 3.5 mm into aluminium. “The engineering challenge associated with Y-90 was first encountered at Three Mile Island, when they realised that the energy of the beta particles from it was sufficiently high to penetrate their personal protective equipment,” he notes.
Do not disturb
These potential biological hazards make it imperative to monitor potential radioactive contamination and address any leakages, and they also provide a basis for in situ monitoring of such leaks. One approach is to extract water or earth samples, often via boreholes, for offsite analysis in a laboratory. Unfortunately, what’s measured in the lab could be completely different to the radiological environment that you’re trying to understand. “This is an example that highlights the fact that trying to measure something actually changes the thing you’re trying to measure,” notes Joyce.
When undisturbed, Sr-90 and Y-90 reach secular equilibrium, a quiescent state in which Y-90 is produced at the same rate as its decay. Y-90 can tend to react with oxygen in the environment, dependent on pH, to form insoluble products such as yttrium oxide, known as yttria, and colloidal carbonate complexes that precipitate out of the surrounding water environment and can combine with calcium and silicon in the surrounding geology.
“There’s a steady-state radioactivity environment because it’s in secular equilibrium, and also a steady-state geochemistry environment associated with how much yttria is in suspension, settled out or stuck in the geology around it,” says Joyce. “But should it be disturbed by manual intervention this might lift plumes of material, redistributing the radioactivity in the area you’re working in. The risk associated with that is different to the risk assessments associated with the quiescent environment.”
PhD opportunity A PhD studentship is available in Lancaster University’s engineering department to study Sr-90 and Y-90 contamination in land and aqueous environments, under Joyce’s supervision. See “Apply now” below for more details. (Courtesy: Lancaster University)
Joyce and his team are taking a different approach, by developing a method to monitor radioactive contamination in situ. The technique exploits the bremsstrahlung radiation generated when high-energy beta particles emitted by Sr-90 and Y-90 interact with their surrounding environment and slow down. And while beta particles only travel a few millimetres before they can no longer be detected, bremsstrahlung radiation comprises far more penetrating X-ray photons that can be measured at much greater distances.
The researchers are also using an astrophysical technique to determine the distribution of the measured radioactivity. The approach uses the Moffat point spread function – developed back in 1969 to find the distribution of galaxies – to analyse the depth and spread of the contamination and, importantly, how it is changing over time.
“If the depth of these radioactive features changes, that tells you whether things are getting worse or better,” Joyce explains. “Put simply, if they’re getting nearer to the surface, that’s probably not something that you want.”
The PhD project
The team has now demonstrated that bremsstrahlung measurements can discriminate the combined Sr-90/Y-90 beta emission from gamma radiation emitted by caesium-137 (another high-yield fission product) during in situ groundwater monitoring. The next goal is to distinguish emissions from the two beta emitters.
As such, Joyce has secured funding from the UK’s Nuclear Decommissioning Authority for a PhD studentship to develop methods to detect and quantify levels of Sr-90 and Y-90 in contaminated land and aqueous environments. The project, based at Lancaster University, also aims to understand the accuracy with which the two radioisotopes can be separated and investigate their respective kinetics.
The first task will be to determine whether bremsstrahlung emissions can discriminate between these two sources of radioactive contamination. Bremsstrahlung is produced in a continuous energy spectrum, with a maximum corresponding to the maximum energy of the beta particles (which also have a continuous energy distribution). Joyce points out that, while it is quite difficult to pinpoint this maximum, it could enable deconvolution of the contributions from Sr-90 and Y-90 to the bremsstrahlung spectrum.
It may also be possible to distinguish the two radioisotopes via direct detection of the beta particles, or a completely different solution may emerge. “Never say never with a PhD,” says Joyce. “There may be a better way of doing it that we’re not aware of yet.”
Joyce emphasizes the key role that such radiation monitoring techniques could play in nuclear decommissioning projects, such as the clean-up of the Dounreay shaft, for example. The 65-m deep shaft and silo were historically used to store radioactive waste from the Dounreay nuclear reactor in Scotland. This waste now needs to be retrieved, repackaged and stored somewhere isolated from people, animals and plants.
As the facility is emptied of radioactive material, the radiological environment will change. Ideally, it will become safer, and uncertainty reduced, with any changes potentially able to inform planning. “With this new technology we’ll be able to monitor radiation levels as the programme progresses, to understand exactly what’s happening in the environment as things are being cleaned up,” explains Joyce.
“The world would be a better place as a result of the ability to make these measurements, and they could inform how similar challenges are dealt with the world over,” Joyce tells Physics World. “If you asked me ‘why should somebody do this PhD?’, altruistically, it’s about taking us closer to the point where our grandchildren don’t have to worry about these things – that’s what’s important.”
Apply now
To find out more about the PhD studentship, which is fully funded for eligible UK students, contact Malcolm Joyce at m.joyce@lancaster.ac.uk. Candidates interested in applying should send a copy of their CV together with a personal statement or covering letter addressing their background and suitability for this project before the closing date of 31 August 2024.
Spatially fractionated radiotherapy is a novel cancer treatment that uses a pattern of alternating high-dose peaks and low-dose valleys to deliver a nonuniform dose distribution. Numerous preclinical investigations have demonstrated that by shrinking the peaks and valleys to submillimetre dimensions, the resulting microbeams confer extreme normal tissue tolerance, enabling delivery of extremely high peak doses and providing excellent tumour control.
The technique has not yet, however, been used to treat patients. Most preclinical studies employed synchrotron X-ray sources, which deliver microbeams at ultrahigh dose rates but are not widely accessible. Another obstacle is that these extremely narrow beams (100 µm or less) are highly sensitive to any motion during irradiation, which can blur the pattern of peak and valley doses.
Instead, a team at the Mayo Clinic in Rochester, Minnesota, is investigating the clinical potential of minibeam radiation therapy (MBRT), which employs slightly wider beams (500 µm or more) spaced by more than 1000 µm. Such minibeams still provide high normal tissue sparing and tumour control, but their larger size and spacing makes them less sensitive to motion. Importantly, minibeams can also be generated by conventional X-ray sources with lower dose rates.
To perform MBRT, the researchers adapted the Xstrahl 300, a clinical orthovoltage unit with 180 kVp output. “Because minibeam radiotherapy uses very narrow beams of radiation spaced very closely together, it requires low-energy orthovoltage X-rays,” Grams explains. “Higher-energy X-rays from linear accelerators would scatter too much and blur the peaks and valleys together.”
The team used cones with diameters between 3 and 10 cm to define the field size and create homogeneous circular fields. This output was then split into minibeams using tungsten collimators with 0.5 mm wide slits spaced 1.1 mm apart.
Commissioning measurements showed that the percentage depth dose decreased gradually with depth, reaching 50% somewhere between 3.5 and 4 cm. Peak-to-valley ratios were highest at the surface and inversely related to cone size. Peak dose rates at 1 cm depth ranged from 110 to 120 cGy/min.
The low dose rate of the orthovoltage system means that treatment times can be quite long and patient motion may be an issue. To mitigate motion effects, the researchers created 3D printed collimator holders that conform to the patient’s anatomy. These holders are fixed to the patient, such that any motion causes the patient and collimator to move together, maintaining the spatial separation of the peak and valley doses.
“This treatment had never been delivered to a human before, so we had to figure out all of the necessary steps in order to do it safely and effectively,” says Grams. “The main challenge is patient motion, which we solved by attaching the collimator directly to the patient.”
First-in-human treatments
The team treated two patients with MBRT. The first had a large (14x14x11 cm) axillary tumour that was causing severe pain and restricted arm motion, prompting the decision to use MBRT to shrink the tumour and preserve normal tissue tolerance for future treatments. He was also most comfortable sitting up, a treatment position that’s only possible using the orthovoltage unit.
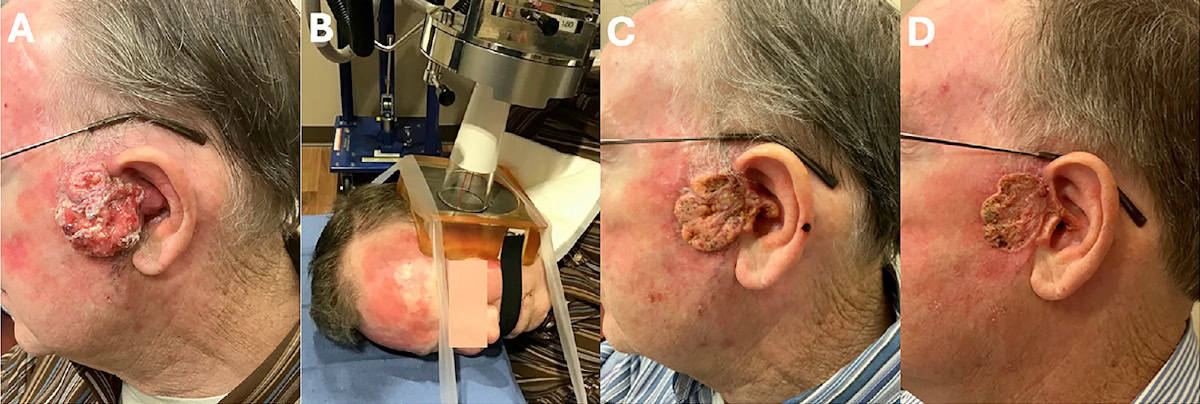
The second patient had a 7x6x3 cm ear tumour that completely blocked his external auditory canal, causing hearing loss, shooting pain and bleeding. He was unable to undergo surgery due to a fear of general anaesthesia and instead was recommended MBRT to urgently reduce pain and bleeding without compromising future therapies.
“These patients had very few treatment options that the attending physician felt would actually help mitigate their symptoms,” explains Grams. “Based on what we learned from our preclinical research, they were felt to be good candidates for MBRT.”
Both patients received two daily MBRT fractions with a peak dose of 1500 cGy at 1 cm depth, using the 10 cm cone for patient 1 and the 5 cm cone for patient 2. The radiation delivery time was 11.5 or 12 min per fraction, with the second fraction delivered after rotating the collimator by 90°.
Treatment response (A) The tumour of patient 2 on the day of MBRT. (B) Treatment photo showing the patient with the collimator holder attached, the 5 cm cone flush and in contact with the tungsten collimator. Tumour response 16 days (C) and 34 days (D) after MBRT. (Courtesy: Int. J. Radiat. Oncol. Biol. Phys. 10.1016/j.ijrobp.2024.06.035)
Prior to treatment, the collimator was attached to the patient and a small piece of Gafchromic film was placed directly on the tumour for in vivo dosimetry. For both patients, the films confirmed the pattern of peak and valley doses, with no evidence of dose blurring.
For patient 1, the measured peak and valley doses were 1900 and 230 cGy, respectively. The expected doses (based on commissioning measurements) were 2017 and 258 cGy, respectively. Patient 2 had measured peak and valley doses of 1800 and 180 cGy, compared with expected values of 1938 and 248 cGy.
Both patients exhibited positive clinical responses to MBRT. Six days after his second treatment, patient 1 reported resolution of pain and improved arm motion. Three weeks later, the tumour continued to shrink and his full range of motion was restored. Despite the 10 cm cone not fully encompassing the large tumour, a uniform decrease in volume was still observed.
After one treatment, patient 2 had much reduced fluid leakage, and six days later, his pain and bleeding had completely abated and his hearing improved. At 34 days after MBRT, he continued to be asymptomatic and the lesion had completely flattened. Pleased with the outcome, the patient was willing to reconsider the recommended standard-of-care resection.
“The next step is a formal phase 1 trial to determine the maximum tolerated dose of minibeam radiotherapy,” Grams tells Physics World. “We are also continuing our preclinical work aimed at combinations of MBRT and systemic therapies like immunotherapy and chemotherapy drugs.”
The practical MR-linac Aurora-RT, a rotating MR-linac that combines a 6 MV linac with a 0.5 T biplanar MRI with a beam stop, is designed to reduce installation and operating costs. (Courtesy: Gino Fallone)
The past few decades have seen MR-guided radiotherapy evolve from an idea on the medical physicists’ wish list to a clinical reality. At the recent AAPM Annual Meeting, experts in the field took a look at three MR-linac systems, the clinical impact of this advanced treatment technology and the potential future trajectory of MR-guided radiotherapy.
Millimetres matter
Maria Bellon from Cedars-Sinai (speaking on behalf of James Dempsey and ViewRay Systems) began the symposium with an update on the MRIdian, an MR-guided radiotherapy system that combines a 6 MV linac with a 0.35 T MRI scanner. She explained that ViewRay Systems was formed in early 2024 to save the MRIdian technology following the demise of ViewRay Technologies.
Bellon described ViewRay’s quest to minimize treatment margins – the region that’s deliberately destroyed outside of the tumour. In radiotherapy, geometric margins are necessarily added to account for microscopic disease or uncertainties. “But millimetres matter when it comes to improving outcomes for cancer patients,” she said.
The MRIdian A3i, the company’s latest platform, is designed to minimize margins and maximize accuracy using three key features: auto-align, auto-adapt and auto-target. Auto-align works by aligning a very sharp beam to high-resolution images of the soft tissues to be targeted or spared. The auto-adapt workflow begins with the acquisition of a high-resolution 3D MRI for localization. Within 30 s, it automatically performs image registration, contour mapping, predicted dose calculation, IMRT plan re-optimization, best plan selection and plan QA.
Once treatment begins, auto-targeting is employed to deal with organ motion. The treatment beam is controlled by the MR images and only turned on when the tumour lies within defined margins. Organ motion can also cause interplay effects, in which the dose distribution contains gaps or areas of overlap that result in hot and cold spots. Larger margins can worsen this effect – another reason to keep them as small as possible.
Decreasing margins The MRIdian MR-linac is designed to minimize treatment margins and maximize accuracy. (Courtesy: James Dempsey/Viewray Systems)
Bellon shared some clinical studies demonstrating how margins matter. The MIRAGE trial, for example, showed that 2 mm margins and MR-guided radiotherapy resulted in significantly lower toxicity for prostate cancer patients than 4 mm margins and CT guidance. Elsewhere, the multicentre SMART trial treated pancreatic cancer with a 3 mm margin, which improved two-year overall survival with few to no higher-grade GI toxicities.
“This is actual evidence that reducing margins, making them real, controlling them, will improve outcomes for patients,” she noted.
Looking to the future, could sub-millimetre margins be achievable? Bellon described how a new head coil and submillimetre-resolution imaging can enable frameless MRI-guided stereotactic radiosurgery (SRS) on the A3i platform. To date, the team has investigated phantoms and healthy volunteers. “I think that it would be a really great advantage of the system to step into the SRS space,” she said.
“Innovation remains at the forefront for ViewRay Systems as they continue to strive to image faster, image in more directions and planes, and use more automation and innovation to control margins and make them smaller than ever,” said Bellon.
Mitigating motion
The second speaker, Bas Raaymakers from UMC Utrecht, discussed the Elekta Unity, a MR-linac envisaged back in 1999 by Raaymakers and his colleague Jan Lagendijk, and designed and built in collaboration with industrial partners Elekta and Philips.
Unity comprises a ring-gantry mounted linac integrated with a 1.5 T MRI. Raaymakers described some of the clinical opportunities conferred by such MR guidance. For starters, high-precision dose delivery with small margins enables use of a lower number of treatment fractions. For adrenal gland and prostate treatments, the Utrecht team has moved from 20 to five fractions, and is studying ultra-hypofractionation to just one or two.
Precise dose delivery also protects organs-at-risk and could enable delivery of higher doses to hard-to-treat cancers, such as pancreatic or renal cell cancer, where surrounding tissues are highly radiosensitive. “This is the future of MR-guided radiotherapy, this gives all kinds of opportunities that we do not have now,” Raaymakers said.
The Unity can track all types of motion – breathing motion, drifts or sudden movements – in real time and in 3D. The system’s comprehensive motion management (CMM) system performs two orthogonal cine MR scans and then uses these scans to perform gating and intrafraction drift correction (in which the treatment centre is changed to correct for drifts). Treatments with CMM began last year and analysis of the first seven patients showed that the gating works and improves conformality.
Raaymakers described how CMM combined with high soft-tissue contrast enables prostate cancer treatments in five fractions with 2 mm margins. To minimize intrafraction motion, a necessity for such small margins, the Utrecht team developed a regime in which a new plan is created halfway through the treatment. This replanning reduced the residual motion at the end of the treatment enough to enable 2 mm margins.
The team also investigated the use of drift correction halfway through the fraction and found that, dosimetrically, it was same as the replanning approach. “The whole effort of replanning can also be done with drift correction,” said Raaymakers. “Now we can do prostate treatment in 30 minutes, with 2 mm margins. This will be used, and we will explore how we can use drift correction for all types of treatment.”
The Elekta Unity Elekta has sold around 150 of its MR-linac systems, with about 85 already in clinical operation. (Courtesy: Elekta)
The ultimate aim, Raaymakers said, is to reach the position where we don’t worry about patient motion at all. For example, is it possible to treat a beating heart? As an example, he described the MEGASTAR study of MR-guided stereotactic arrythmia radioablation, in which MRI is used to follow the beating heart and MLC tracking employed to accurately hit the target.
Raaymakers concluded with a look at the future impact of MR-guided radiotherapy. He noted that radiotherapy is a low-cost technology used to treat 50% of all cancer patients and that MR guidance can improve it further, via hypofractionation, smarter workflows, smaller margins and reduced toxicity.
“I think this is an option to shift from invasive treatments towards radiotherapy; we can postpone surgery for certain patients or omit surgery for others,” he said. “This is something we should strive for in MR-guided radiotherapy, to make this message clear to the rest of the oncology world.”
The practical MR-linac
The final speaker in the symposium was Gino Fallone from the Cross Cancer Institute (CCI), the University of Alberta and MagnetTx Oncology Solutions. Fallone introduced the Aurora-RT, a rotating MR-linac that combines a 6 MV linac with a 0.5 T biplanar MRI with a beam stop. The system was first prototyped in 2008 and is now FDA approved and CE Marked.
The unique feature of the Aurora-RT is that it can be used in two configurations: with horizontal magnets and the beam perpendicular to the magnetic field, or vertical magnets with the beam parallel to B0. Fallone noted that the parallel configuration is the clinical product as it significantly reduces dose perturbations and enables large 3D couch shifts
Fallone told the audience why MagnetTx chose to use 0.5 T MRI. Knowing that the system would require fast imaging techniques, such as bSSFP (balanced steady-state free precession), the team assessed the contrast-to-noise ratio for bSSFP at various field strengths, and found that it was greatest at 0.5 T. “While image quality is determined by the signal-to-noise ratio, which does go up with magnetic field, contrast-to-noise is also critical,” he explained.
The Aurora-RT has a wide bore of 110 x 60 cm, reducing patient claustrophobia and increasing throughput. This large opening also enables significant couch motion of ±23 cm in the vertical and lateral directions, allowing treatments to be performed in the same way as conventional radiotherapy and improving the clinical flow. “You can place the target at the planned location every time, you don’t have to do online replanning for every single patient,” said Fallone. “Such a large couch motion also allows isocentric treatment of peripheral targets.”
To track and treat moving organs, the CCI researchers developed a technique called NifteRT, or non-invasive intrafraction tumour tracked radiotherapy. The approach involves MR imaging at 4 frames/s, autocontouring, and tumour motion prediction for each patient. The predicted tumour position is then used to control the MLC to shape and position the beam to the target.
Fallone emphasized that the team employs a lot of AI and deep learning. “This allowed us to do faster imaging without creating distortions, it allowed us to do very accurate segmentation and it allowed us to do tumour tracking with prediction and irradiation,” he explained.
The Aurora-RT was designed with simplicity and cost reduction in mind. The system can be sited in any typically sized vault, installed through the vault door maze, and does not require a cryogen exhaust vent. Because the Aurora-RT has a beamstop, shielding is required only for scattered radiation, reducing site costs. Once installed, the system runs without needing liquid helium or any liquid cryogens, reducing operating costs. The magnet can be turned on or off in minutes, improving research and service operations. It also uses many existing radiotherapy techniques, for example, existing ion chambers, laser setup and table shifts.
Fallone concluded that the Aurora-RT offers increased throughput, decreased claustrophobia, no process changes, significantly reduced dose perturbations for safer delivery and improved MR guidance via use of the 0.5 T “sweet spot”. Simplified installation in any vault, without the need for an exhaust vent or shielding for the primary radiation beam, decreases installation and operating costs.
Prove its worth
Having discussed the advantages of and clinical evidence for MR-guided radiotherapy, the speakers were asked why MR-linacs still only comprise 2% of the market and why users appear slow to adopt this approach.
“Throughput is a constant conversation that we’re having, despite the fact that yearly throughput tends to be high because a lot of treatments can be hypofractionated,” said Bellon. “On-table adaptive is very intimidating for people, but I don’t know why it’s still considered a niche treatment.”
Raaymakers believes that the conservatism of the medical field is working against them. “Right now, it’s a lot of hassle and there’s no proof…We have to prove that it’s really worth it and hopefully then adoption will get faster.”
Fallone suggests that medical physicists are too scared of MR and that MR-linacs are still too expensive. “We know MRI is better than CT, now we have to convince the bosses,” he said. “If you get a better image you will treat better; there’s nothing to prove.”
Gamma imaging is a nuclear medicine technique employed in over 100 different diagnostic procedures. Also known as scintigraphy, the approach uses gamma cameras to image the distribution of gamma-emitting radiopharmaceuticals administered to the body, with applications including thyroid imaging, tumour imaging, and lung and renal studies.
Most clinical gamma cameras are large devices designed for whole-body scanning and located in their own dedicated room. While such systems offer high sensitivity and a large field-of-view (FOV), they are not ideal for patients who cannot attend the nuclear medicine department. A small gamma camera, on the other hand, could enable scanning of more patients in far more scenarios.
Made to meet this challenge, Seracam is a new portable gamma camera developed and designed by UK medical imaging company Serac Imaging Systems. Just 15 cm in diameter, 24 cm long and weighing 5 kg, the hybrid optical–gamma camera is designed for small-organ imaging within outpatient clinics, intensive care units, or even in operating theatres during surgery.
“Gamma imaging is no longer confined to the nuclear medicine department,” explains Sarah Bugby from Loughborough University. “The system has a much smaller footprint, it could be stored in a cupboard and brought out only when needed.”
Bugby and colleagues have now performed a detailed assessment of Seracam’s clinical potential, reporting their findings in EJNMMI Physics.
System evaluation
Seracam uses a CsI(Tl) crystal scintillator to convert incoming gamma photons to optical photons. This light is then captured by a 25.5 x 25.5 mm detector, divided into 245 x 245 pixels, and analysed in real time to create an image of the gamma counts.
Hybrid optical–gamma camera The compact Seracam from Serac Imaging Systems. (Courtesy: CC BY 4.0/EJNMMI Phys. 10.1186/s40658-024-00659-7)
The camera integrates four pinhole collimators, with pinhole diameters of roughly 1, 2, 3 and 5 mm. The physics of collimation means that smaller pinhole diameters provide better spatial resolution but lower sensitivity, while larger pinholes provide higher sensitivity but with a trade-off in image resolution.
“With Seracam, you can change the collimator at the press of a button in just a second or so,” Bugby explains. “In traditional gamma cameras, collimators must be changed manually, which is time consuming as they’re about 60 cm square and made of lead. This means that, when imaging a patient, you’re locked into the initial collimator choice. Seracam offers the flexibility to adjust these trade-offs on the fly.”
Another novel feature is Seracam’s hybrid gamma and optical imaging. A gamma image simply comprises bright spots on a dark background, there are no anatomical landmarks for context. Seracam overlays the optical and gamma images to show both gamma and anatomical information.
Bugby and colleagues evaluated Seracam in a series of performance tests using 99mTc – the most common isotope used in nuclear medicine. Measurements of parameters including spatial resolution, sensitivity and image uniformity demonstrated that the device is suitable for clinical use.
Clinical scenarios
Next, the team performed experimental simulations of two clinical scenarios: thyroid imaging, used to assess the function of thyroid tissue, nodules and tumours; and a gastric emptying study, used to time stomach emptying after ingestion of a radiolabelled meal.
For thyroid imaging, the researchers examined a Picker phantom, an acrylic block with a thyroid-shaped well filled with 99mTc. They also imaged a head-and-neck phantom with fillable head and thyroid volumes, simulating hyperthyroidism and a normal thyroid with a hot nodule.
Seracam produced good quality images for both phantoms, showing its suitability for thyroid scintigraphy. The researchers note that the Picker phantom image quality was similar to that achieved with a traditional large-FOV camera, but using significantly lower counts and a larger imaging distance than employed in a clinical setting.
Hyperthyroidism simulation Hybrid Seracam images acquired using 1, 3 and 5 mm collimators show the thyroid shape, location and activity distribution. The smaller pinholes enhance spatial resolution, but at the expense of photon statistics. (Courtesy: CC BY 4.0/EJNMMI Phys. 10.1186/s40658-024-00659-7)
For gastric emptying, the team simulated a human stomach using a 500 ml flask filled with 99mTc and gradually emptied via syringes. At each emptying step, Seracam acquired a 120 s image using the 5.00 mm pinhole. The simulation showed that Seracam could produce a gastric emptying curve with the expected linearity at clinically relevant activities.
“We intentionally chose challenging rather than best-case scenarios, so the fact that we saw good performance is a really strong indicator,” says Bugby. “Gastric emptying isn’t a small-organ scenario, so in this case Seracam outperformed our expectations. Of course, this all needs to be validated in the clinic.”
The team concludes that Seracam can provide effective small-FOV gamma imaging within a clinical setting with excellent spatial resolution, although with reduced sensitivity compared with large-FOV devices. “Our results show that Seracam is well suited for the kinds of clinical tests it was designed for,” Bugby points out.
Seracam’s small camera head can be positioned in places that larger camera heads on conventional systems cannot reach. This flexibility in positioning could itself improve image quality: moving the camera closer to the patient helps compensate for the sensitivity that’s sacrificed by making such a small device.
“Combining this manoeuvrability with other beneficial features unavailable in large FOV systems, such as hybrid gamma–optical imaging and instant collimator changes, opens up new approaches to imaging,” says Bugby. “It’s easy to imagine a scenario that begins in a high-sensitivity ‘survey mode’ before switching to a high-resolution ‘imaging mode’ to investigate identified uptake sites. We’re excited to see how experienced clinicians will take advantage of these novel features.”
The researchers are now simulating other clinical applications, such as sentinel lymph node biopsy, and Seracam is being trialled at clinical sites in the US and Malaysia. Co-funded by the UK’s innovation agency, Innovate UK, Loughborough University researchers are also working on new image analysis and display techniques to enable Seracam’s use in radioguided surgery.
“We’re hopeful that these new innovations will be trialled by a team at the University of Malaya Medical Centre and others very soon,” Bugby tells Physics World.
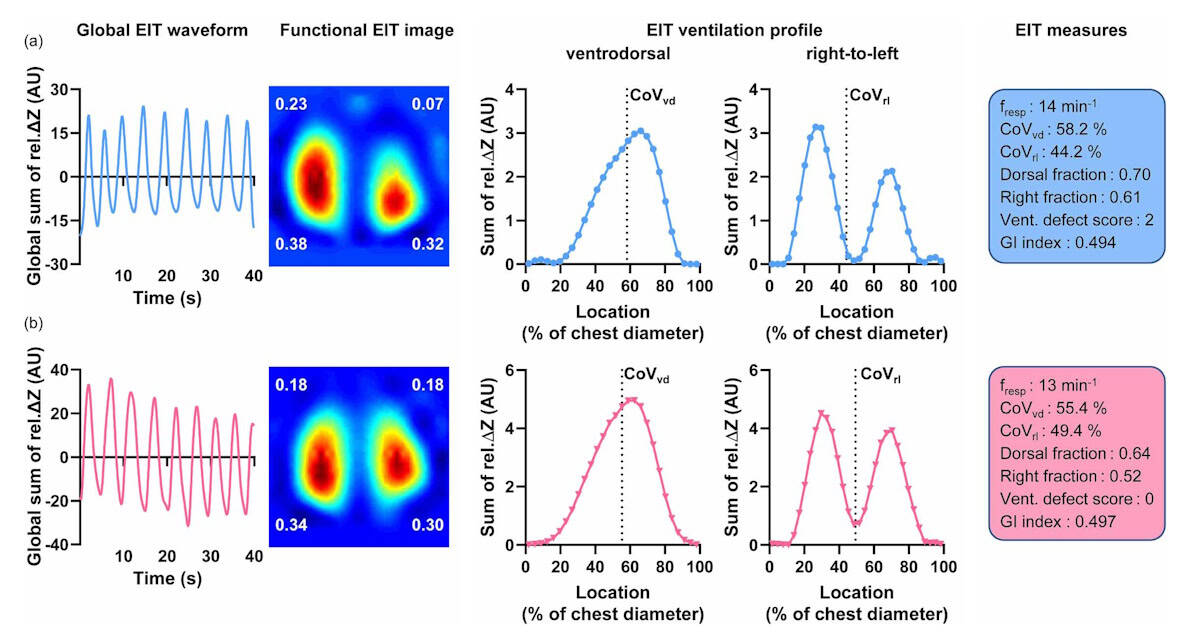
Key differences Example EIT exams in a man (a) and a woman (b). The waveforms show the tidal variation of the EIT signal, while the images show the distribution of tidal impedance variation (the numbers represent the ventilation fraction in each quadrant). The profiles show the distribution of ventilation in the front-to-back and right-to-left directions. The boxes on the right present parameters derived from the EIT data. (Courtesy: I Frerichs et al Physiol. Meas. 10.1088/1361-6579/ad5ef7)
Electrical impedance tomography (EIT) is a radiation-free, non-invasive imaging technique that uses measurements from surface electrodes to create a tomographic image of the body. EIT is particularly suited to assessing lung function: while conventional radiological imaging reveals lung morphology, EIT can be used to directly monitor regional lung ventilation and perfusion, and track changes due to disease or therapy.
To date, however, few EIT studies have examined the respiratory differences between men and women. To address this shortfall, a team from the University Medical Centre Schleswig-Holstein in Kiel, Germany has performed a detailed study of large group of volunteers to investigate how biological sex affects EIT measurements. Their findings suggest that key differences exist, and that these must be considered when interpreting clinical chest EIT studies.
“The anatomical and physiological differences between women and men make it important to determine sex differences in medical research,” explains first author Inéz Frerichs. “The relative lack of studies on sex-dependent differences in EIT findings is related to the fact that the method is not so old and large population studies in this field still need to be conducted. Small pilot studies do not have the power to establish possible differences reliably.”
Detailed data analysis
EIT works by applying small alternating currents through pairs of electrodes attached to the skin near the organ being examined. Measuring the resulting voltage differences through all adjacent electrode pairs enables construction of a 2D tomographic map of the electrical conductivity of that body part.
In their latest study, described in Physiological Measurement, Frerichs and colleagues analysed data from 218 adults with no known lung disorders who had participated in a previous EIT study. The cohort included 120 men and 98 women, with no significant differences between the subgroups asides height and weight. The team examined EIT recordings obtained during about one minute of quiet relaxed breathing (known as tidal breathing), with the subject seated.
The EIT exams were performed using an array of 16 electrodes placed around the lower chest, with the reference electrode attached onto the belly. Data were acquired at a rate of 33 images/s – a high scan rate that allows continuous assessment of dynamic physiological processes.
For all subjects, the researchers calculated the tidal impedance variation (TIV) for each image pixel in each recorded tidal breath and created 2D plots showing the distribution of tidal volume in the chest cross-section. They then quantified this spatial distribution using a series of established EIT measures: the centre of ventilation in the ventrodorsal (front-to-back) direction (CoVvd) and the right-to-left direction (CoVrl); and the dorsal and right fractions of ventilation.
The overall results from the male and female subgroups revealed significant differences in ventilation distribution between men and women. In the right-to-left direction, women exhibited a more symmetric distribution between the right and left lung regions than men, with CoVrl located more at the right side of the chest in male subjects than in female subjects. The right fraction of ventilation was also higher in men than in women.
Differences were less pronounced in the front-to-back direction, but still significant, with CoVvd predominantly located in the dorsal image half in both sexes, but more dorsally in men.
The researchers also calculated ventilation defect scores, a parameter that further defines the heterogeneity in ventilation distribution throughout the lungs. To calculate this score, they determined the fraction of ventilation in each image quadrant, and assigned a value of 0 (for a fraction of 0.15 or higher), 1 (between 0.10 and 0.15) or 2 (lower than 0.10) to each. Summing the four quadrant values gave the overall ventilation defect score.
They observed that ventilation distribution among quadrants was less heterogeneous in women than in men, with 83.4% of women exhibiting low ventilation defect scores (0 or 1), compared with 57.5% of men. A score higher than 1 was found in 42.5% of men but only in 16.6% of women.
Differences matter
The researchers conclude that ventilation distribution detected by EIT is affected by biological sex in this large group of quietly breathing male and female subjects, with the most striking variation the significantly higher right-to-left asymmetry seen in men than in women. They attribute this finding in part to differences in chest anatomy – the left ventricle is much larger in men than in women, even after normalization to body height.
Another possible cause may be breathing mechanics: differences in skeletal chest anatomy mean that women mainly perform thoracic breathing whereas men mainly exhibit abdominal breathing, which creates larger diaphragm motion. As EIT is sensitive to out-of-plane impedance changes, measurements may be affected by the movement of abdominal organs lying above and below the examination plane, particularly as this study used electrodes located at the lower part of the chest. But as the researchers did not monitor the type of breathing during the study, they cannot determine the exact role of this factor.
The findings reiterate the importance of accounting for biological gender when interpreting clinical chest EIT studies. The researchers point out the need for further clinical studies in lung-healthy subjects. “We need to perform large population studies to determine the reference values of several EIT measures for both sexes and also to clarify if sex differences exist when EIT examinations are performed in different body positions and chest sections,” Frerichs tells Physics World.