As well as giving them valuable practical experience of creating an event featuring businesses in the burgeoning quantum sector, it also lets them build links with the very firms they – and the students and postdocs who attended – might end up working for.
A clever win-win if you like, with the day featuring talks, panel discussion and a careers fair made up companies such as Applied Quantum Computing, Duality, Hamamatsu, Orca Computing, Phasecraft, QphoX, Riverlane, Siloton and Sparrow Quantum.
IOP Publishing featured too with Antigoni Messaritaki talking about her journey from researcher to senior publisher and Physics World features and careers editor Tushna Commissariat taking part in a panel discussion on careers in quantum.
The importance of communication and other “soft skills” was emphasized by all speakers in the discussion, but what struck me most was a comment by Carrie Weidner, a lecturer in quantum engineering at Bristol, who underlined that it’s fine – in fact important – to learn to fail.
“If you’re resilient and can think critically, you can do anything,” said Weidner, who is also director of the quantum-engineering CDT. She warned too of the dangers of generative AI, joking that “every time you use ChatGPT, your brain is atrophying”.
Breaking barriers Diya Nair explains the aims and activities of Girls in Quantum (Courtesy: Matin Durrani)
Another great talk was by Diya Nair, a computer-science undergraduate at the University of Birmingham, who is head of global outreach and UK ambassador for Girls in Quantum.
The organization is now active in almost 70 countries around the world, with the aim of “democratizing quantum education”. As Nair explained, Girls in Quantum does everything from arrange quantum computing courses and hackathons to creating its crowdfunded quantum-computing game called Hop.
The event also included a discussion about taking quantum research “from concept to commercialization”. It featured Jack Russel Bruce from Universal Quantum, Euan Allen from eye-imaging tech firm Siloton, Joe Longden from Duality Quantum Photonics, and Stewart Noakes, who has mentored numerous companies over the years.
Noakes emphasized that all high-tech firms have three main needs: talent, money and ideas. In fact, as he explained, companies can sometimes suffer from having too much money as well as too little, especially if they grow too fast and hire people on big salaries who might then need to be let go if funding dries up.
Bruce, though, was positive about the overall state of the quatum-tech sector. “For me, the future is bright,” he said. But as all speakers underlined, if you want to join the industry, make sure you’ve got good communciation skills, an open-minded attitude – and a willingness to learn on the go.
If you’d like more information about careers in quantum, do check out the 2026 Physics World Careers Guide (now in its 10th year) and explore Physics World Jobs, which has up-to-date vacancies across physics.
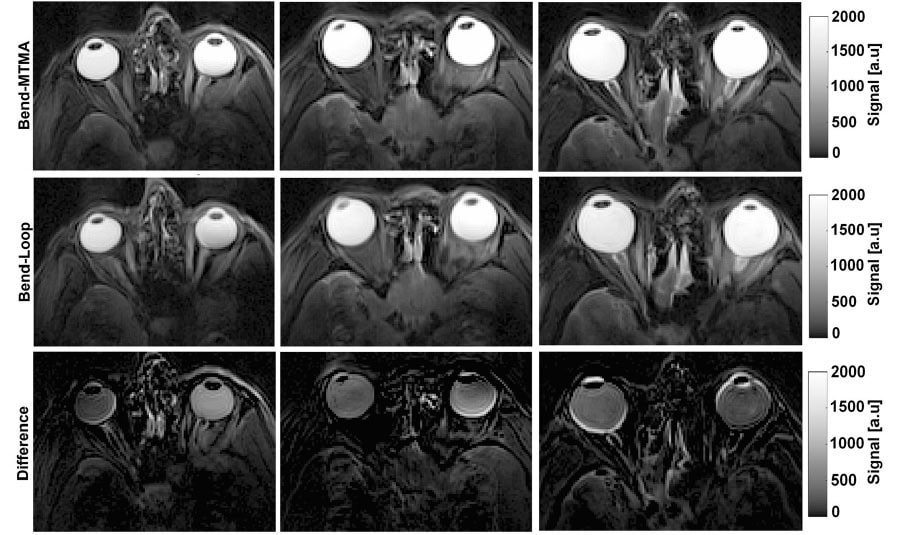
In vivo imaging T2-weighted MRI of three healthy volunteers (left to right columns) using the bend-MTMA and bend-loop antennas reveals increased intraocular signal for the metamaterial-based bend-MTMA configuration. (Courtesy: CC BY 4.0/Advanced Materials 10.1002/adma.202517760)
MRI is one of the most important imaging tools employed in medical diagnostics. But for deep-lying tissues or complex anatomic features, MRI can struggle to create clear images in a reasonable scan time. A research team led by Thoralf Niendorf at the Max Delbrück Center in Germany is using metamaterials to create a compact radiofrequency (RF) antenna that enhances image quality and enables faster MRI scanning.
Imaging the subtle structures of the eye and orbit (the surrounding eye socket) is a particular challenge for MRI, due to the high spatial resolution and small fields-of-view required, which standard MRI systems struggle to achieve. These limitations are generally due to the antennas (or RF coils) that transmit and receive the RF signals. Increasing the sensitivity of these antennas will increase signal strength and improve the resolution of the resulting MR images.
To achieve this, Niendorf and colleagues turned to electromagnetic metamaterials – artificially manufactured, regularly arranged structures made of periodic subwavelength unit cells (UCs) that interact with electromagnetic waves in ways that natural materials do not. They designed the metamaterial UCs based on a double-square split-ring resonator design, tailored for operation at a high magnetic field strength of 7.0 T.
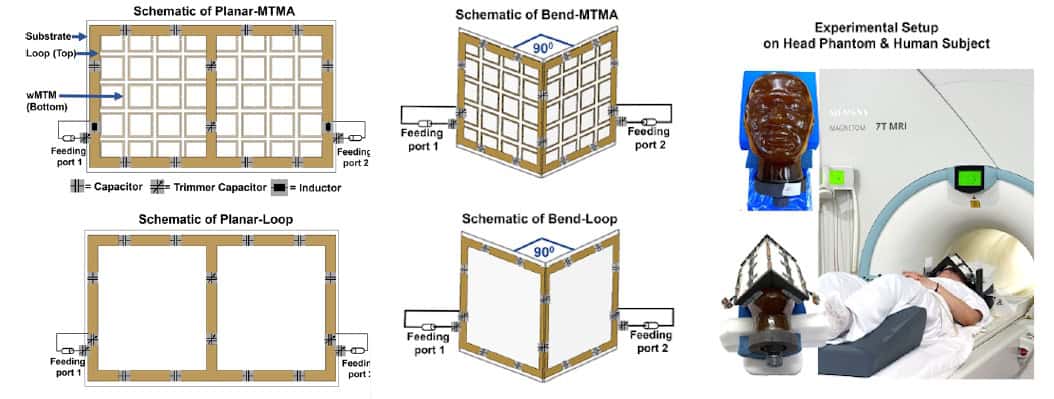
In their latest study, led by doctoral student Nandita Saha and reported in Advanced Materials, the researchers created a metamaterial-integrated RF antenna (MTMA) by fabricating the UCs into a 5 x 8 array. They built two configurations: a planar antenna (planar-MTMA); and a version with a 90° bend in the centre (bend-MTMA) to conform to the human face. For comparison, they also built conventional counterparts without the metamaterial (planar-loop and bend-loop).
The researchers simulated the MRI performances of the four antennas and validated their findings via measurements at 7.0 T. Tests in a rectangular phantom showed that the planar-MTMA demonstrated between 14% and 20% higher transmit efficiency than the planar-loop (assessed via B₁+ mapping).
They next imaged a head phantom, placing planar antennas behind the head to image the occipital lobe (the part of the brain involved in visual processing) and bend antennas over the eyes for ocular imaging. For the planar antennas, B₁+ mapping revealed that the planar-MTMA generated around 21% (axial), 19% (sagittal) and 13% (coronal) higher intensity than the planar-loop. Gradient-echo imaging showed that planar-MTMA also improved the receive sensitivity, by 106% (axial), 94% (sagittal) and 132% (coronal).
Antenna design and deployment Layout of the planar and bend antennas, and the experimental setups for imaging an anatomical head phantom and a volunteer in a 7.0 T whole-body MRI system. (Courtesy: CC BY 4.0/Advanced Materials 10.1002/adma.202517760)
The bend antennas exhibited similar trends, with B₁+ maps showing transmit gains of roughly 20% for the bend-MTMA over the bend-loop. The bend-MTMA also outperformed the bend-loop in terms of receive signal intensity, by approximately 30%.
“With the metamaterials we developed, we were able to guide and modulate the RF fields generated in MRI more efficiently,” says Niendorf. “By integrating metamaterials into MRI antennas, we created a new type of transmitter and detector hardware that increases signal strength from the target tissue, improves image sharpness and enables faster data acquisition.”
In vivo imaging
Importantly, the new MRI antenna design is compatible with existing MRI scanners, meaning that no new infrastructure is needed for use in the clinic. The researchers validated their technology in a group of volunteers, working closely with partners at Rostock University Medical Center.
Before use on human subjects, the researchers evaluated the MRI safety of the four antennas. All configurations remained well below the IEC’s specific absorption rate (SAR) limit. They also assessed the bend-MTMA (which showed the highest SAR) using MR thermometry and fibre optic sensors. After 30 min at 10 W input power, the temperature increased by about 1.5°C. At 5 W, the increase was below 0.5°C, well within IEC safety thresholds and thus used for the in vivo MRI exams.
The team first performed MRI of the eye and orbit in three healthy adults, using the bend-loop and bend-MTMA antennas positioned over the eyes. Across all volunteers, the bend-MTMA exhibited better transmit performance in the ocular region that the bend-loop.
The bend-MTMA antenna also generated larger intraocular signals than the bend-loop (assessed via T2-weighted turbo spin-echo imaging), with signal increases of 51%, 28% and 25% in the left eyes, for volunteers 1, 2 and 3, respectively, and corresponding gains of 27%, 26% and 29% for their right eyes. Overall, the bend-MTMA provided more uniform and higher-intensity signal coverage of the ocular region at 7.0 T than the bend-loop.
To further demonstrate clinical application of the bend-MTMA, the team used it to image a volunteer with a retinal haemangioma in their left eye. A 7.0 T MRI scan performed 16 days after treatment revealed two distinct clusters of structural change due to the therapy. In addition, one of the volunteer’s ocular scans revealed a sinus cyst, an unexpected finding that showed the diagnostic benefit of the bend-MTMA being able to image beyond the orbit and into the paranasal sinuses and inferior frontal lobe.
The team used the planar antennas to image the occipital lobe, a clinically relevant target for neuro-ophthalmic examinations. The planar-MTMA exhibited significantly higher transmit efficiency than the planar-loop, as well as higher signal intensity and wider coverage, enhancing the anatomical depiction of posterior brain regions.
“Clearer signals and better images could open new doors in diagnostic imaging,” says Niendorf. “Early ophthalmology applications could include diagnostic confirmation of ambiguous ophthalmoscopic findings, visualization and local staging of ocular masses, 3D MRI, fusion with colour Doppler ultrasound, and physio-metabolic imaging to probe iron concentration or water diffusion in the eye.”
He notes that with slight modifications, the new antennas could enable MRI scans depicting the release and transport of drugs within the body. Their geometry and design could also be tuned to image organs such as the heart, kidneys or brain. “Another pioneering clinical application involves thermal magnetic resonance, which adds a thermal intervention dimension to an MRI device and integrates diagnostic guidance, thermal treatment and therapy monitoring facilitated by metamaterial RF antenna arrays,” he tells Physics World.
Humans are generating more data than ever before. While much of these data do not need to be stored long-term, some – such as scientific and historical records – would ideally still be retrievable in decades, or even centuries. The problem is that modern digital archive systems such as hard disk drives do not last that long. This means that data must regularly be transferred to new media, which is costly and time-consuming.
A team at Microsoft Research now claims to have found a solution. By using ultrashort, intense laser pulses to “write” data units called phase voxels into glass chips, the team says it has created a medium that could store 4.8 terabytes (TB) of data error-free for more than 10::000 years – a span that exceeds the age of history’s oldest surviving written records.
Direct laser writing
The idea of writing data into glass or other durable media with lasers is not new. Direct laser writing, as it is known, involves focusing high-power pulses, usually just femtoseconds (10-15 s) long, on a three-dimensional region within a medium. This modifies the medium’s optical properties in that region, and each modified region becomes a data-storage unit known as a voxel, which is the 3D equivalent of a pixel.
Because the laser’s energy is focused on a very small volume, the voxels created with this method can be very densely packed. Changing the amplitude and polarization of the laser’s output changes what information gets encoded at each voxel, and an optical microscope can “read out” this information by picking up changes in the light as it passes through each modified region. In terms of the media used, glass is particularly promising because it is thermally and chemically stable and is robust to moisture and electromagnetic interference.
Direct laser writing does have some limitations, however. In particular, encoding information generally requires multiple laser pulses per voxel, restricting the technique’s throughput and efficiency.
Two types of voxel, one laser pulse
Microsoft Research’s “Project Silica” team says it overcame this problem by encoding information in two types of voxel: phase voxels and birefringent voxels. Both types involve modifying the refractive index of the medium, and thus the speed of light within it. The difference is that whereas phase voxels create an isotropic change in the refractive index, birefringent voxels create an anisotropic change by rotating the voxel in the plane of the 120-mm square, 2-mm-thick glass chip.
Crucially, both types of voxel can be produced using a single laser pulse. According to Project Silica team leader Richard Black, this makes the modified region smaller and more uniform, minimizing effects such as light scattering that can interfere with read-outs from neighbouring voxels. It also allows many voxel layers to be written into, and then read out from, a single glass chip. The result is a system that can generate up to 10 million voxels per second, which equates to 25.6 million bits of data per second (Mbit s−1).
Performance of different types of glass
The Microsoft researchers studied two types of glass, both of which have better mechanical properties than ordinary window glass. In 301 layers of fused silica glass, they achieved a data density of 1.59 Gbit mm−3 using birefringent voxels, with a write throughput of 25.6 Mbit s−1 and a write efficiency of 10.1 nJ per bit. In 258 layers of borosilicate glass, the data density reached 0.678 Gbit mm−3 using phase voxels. Here, the write throughput was 18.4 Mbit s−1 and the write efficiency 8.85 nJ per bit.
“The phase voxel discovery in particular is quite notable because it lets us store data in ordinary borosilicate glass, rather than pure fused silica; do it with a single laser pulse per voxel; and do it highly parallel in close proximity,” says Black. “That combination of cheaper material and much simpler and faster writing and reading was a genuinely exciting moment for us.”
The researchers also showed that they could directly inscribe the glass using four independent laser beams in parallel, further increasing the write speeds for both types of glass.
Surviving “benign neglect”
To determine how long these inscribed glass plates could store data, the team repeatedly heated them to 500 °C, simulating their long-term ageing at lower temperatures. The results of these experiments suggest that encoded data could be retrieved after 10::000 years of storage at 290 °C. However, Black acknowledges that this figure does not account for external effects such as mechanical stress or chemical corrosion that could degrade the glass and the data it stores. Another unaddressed challenge is that storage capacity and writing speed will both need to grow before the technology can compete with today’s data centres.
If these deficiencies can be remedied, Black thinks the clearest potential applications would be in national libraries and other facilities that store scientific data and cultural records. “It’s also compelling for cloud archives where data is written once and kept indefinitely,” Black says. He points out that the team has already demonstrated proofs of concept with Warner Bros., the Global Music Vault and the Golden Record 2.0 project, a “cultural time capsule” inspired by the literal golden records launched on the Voyager spacecraft in the 1970s.
A common factor across all these organizations, Black explains, is that they need media that can survive “benign neglect” – something he says Project Silica delivers. He adds that the project also provides what he calls operational proportionality, meaning that its costs are primarily a function of the operations performed on the data, not the length of time the data are kept. “This completely alters the way we think about keeping archival material,” he says. “Once you have paid to keep the data, there is little point in deleting it, and you might as well keep it.”
Microsoft began exploring direct laser data storage in glass nearly a decade ago thanks to team member Ant Rowstron, who recognized the potential of work being done by physicist Peter Kazansky and colleagues at the University of Southampton, UK. The latest version of the technique, which is detailed in Nature, grew out of that collaboration, and Black says its capabilities are limited only by the power and speed of the femtosecond laser being used. “We have now concluded our research study and are sharing our results so that others may build on our work,” he says.
“Surround sound for biological cells,” is how Luke Cox describes the ultrasound technology that Impulsonics has developed to solve the “unsticking problem” in biomedical science. Cox is co-founder and chief executive of UK-based Impulsonics, which spun-out of the University of Bristol in 2023.
He is also my guest in this episode of the Physics World Weekly podcast. He explains why living cells grown in a petri dish tend to stick together, and why this can be a barrier to scientific research and the development of new medical treatments.
The system uses an array of ultrasound transducers to focus sound so that it frees-up and manipulates cells in a way that does not alter their biological properties. This is unlike chemical unsticking processes, which can change cells and impact research results.
We also chat about Cox’s career arc from PhD student to chief executive and explore opportunities for physicists in the biomedical industry.
The following articles are mentioned in the podcast:
An analysis of more than 5.2 million papers in 5000 different journals has revealed a dramatic rise in the use of artificial intelligence (AI) tools in academic writing across all scientific disciplines, especially physics.
However, the analysis has revealed a big gap between the number of researchers who use AI and those who admit to doing so – even though most scientific journals have policies requiring the use of AI to be disclosed.
Carried out by data scientist Yi Bu from Peking University and colleagues, the analysis looks at papers that are listed in the OpenAlex dataset and were published between 2021 and 2025.
To assess the impact of editorial guidelines introduced in response to the growing use of generative AI tools such as ChatGPT, they examined journal AI-writing policies, looked at author disclosures and used AI to see if papers had been written with the help of technology.
The AI detection analysis reveals that the use of AI writing tools has increased dramatically across all scientific disciplines since 2023. It also finds that 70% of journals have adopted AI policies, which primarily require authors to disclose the use of AI-writing tools.
IOP Publishing, which publishes Physics World, for example, has a journals policy that supports authors who use AI in a “responsible and appropriate” manner. It encourages authors, however, to be “transparent about their use of any generative AI tools in either the research or the drafting of the manuscript”.
A new framework
But in the new study, a full-text analysis of 75 000 papers published since 2023, reveals that only 76 articles (about 0.1% of the total) explicitly disclosed the use of AI writing tools.
In addition, the study finds no significant difference in the use of AI between journals that have disclosure policies and those that do not, which suggests that disclosure requirements are being ignored – what the authors call a “transparency gap”.
The study also finds that researchers from non-English-speaking countries are more likely to rely on AI writing tools than native English speakers. Increases in the use of AI writing tools are found to be particularly rapid in journals with high levels of open-access publishing.
The authors now call for a re-evaluation of ethical frameworks to foster responsible AI integration in science. They state that prohibition or disclosure requirements are insufficient to regulate AI use, with their results showing that researchers are not complying with policies.
The authors argue that instead of “opposition and resistance”, “proactive engagement and institutional innovation” is needed “to ensure AI technology truly enhances the value of science”.
Humanity has had a complicated relationship with machines and technology for centuries. While we created these inventions to make our lives easier, and have become heavily reliant upon them, we have often feared their impact on society.
In her debut book, The Body Digital: a Brief History of Humans and Machines from Cuckoo Clocks to ChatGPT, Vanessa Chang tells the story of this symbiotic partnership, covering tools as diverse as the self-playing piano and generative AI products. The short book combines creative storytelling, an inward look at our bodies and interpersonal relationships, and a detailed history of invention. Chang – who is the director of programmes at Leonardo, the International Society for the Arts, Sciences, and Technology in California – offers us a framework for examining future worlds based on the relationship between humanity and machines.
“Technology” has no easy definition. The Body Digital therefore takes a broad approach, looking at software, machines, infrastructure and tools. Chang examines objects as mundane as the pen and as complex as the road networks that define our cities. She focuses on the interplay between machine and human: how tools have lightened our load and become embedded in our behaviour. In doing this she asks the reader: is it possible for the human body to extract itself from technology?
Each chapter of the book centres on a different part of the human anatomy – hand, voice, ear, eye, foot, body and mind – looking at the historical relationship between that body part and technology. Chang follows this thread through to the modern day and the large-scale impact these technologies have had on the development of our communities, communications and social structures. The chapters are a vehicle for Chang to present interesting pieces of history and discussions about society and culture. Her explanations are tightly knit, and the book covers huge ground in its relatively concise page count.
Chang avoids “doomerism”, remaining even-handed about our reservations towards technological advancement. She is careful in her discussion of new technology, particularly those that are often fraught in the public discourse, such as the use of generative AI in creating art, and the potential harms of facial-recognition software.
She includes genuine concerns – like biases creeping into training data for large language models – but mitigates these fears by discussing how technologies have become enmeshed in human culture through history. Our fear of some technologies has been unfounded – take, for example, the idea that the self-playing piano would supersede live piano concerts. These debates, Chang argues, have happened throughout the history of technology, and some of the same arguments from the past can easily be applied to future technology.
While this commentary is often thought-provoking, it sometimes doesn’t go as far as it might. There is relatively limited discussion throughout the book about the technological ecosystem we currently live in and how that might impact our level of optimism about the future. In particular, the topics of human labour being supplanted by machine labour, and the impacts of tech monoliths like Apple and Google, are relatively minimal.
In one example, Chang discusses the ways in which “telecommunication technologies might serve as channels into the afterlife”, allowing us to use technology to artificially recreate the voices of our loved ones after death. While the book contains a full discussion of how uncanny and alarming this type of “artistic necrophilia” might be, Chang tempers fear by pointing out that by being careful with our data, careful with our digital selves, we might be able to “mitigate the transformation of [our] voices into pure commodities”. However, the questions of who controls our data, the relationship between data and capital, and the level of control that we have over the use of our data, is somewhat limited.
Poetic technology
The difference between offering interesting ideas and overexplaining is a hard needle to thread, and one that Chang navigates successfully. One striking feature of The Body Digital is the quality of the prose. Chang has a background in fiction writing and her descriptions reflect this. An automaton is anthropomorphized as a “petite, barefoot boy” with a “cloud of brown hair”; and the humble footpath is described as “veer[ing] at a jaunty angle from the pavement, an unruly alternative to concrete”. As a consequence, her ideas are interesting and memorable, making the book readable and often moving.
Particularly impressive is Chang’s attitude to exposition, which mimics fiction’s age-old adage of “show, don’t tell”. She gives the reader enough information to learn something new in context and ask follow-up questions, without banging the reader over the head with an answer to these questions. The book mimics the same relationship between the written word and human consciousness that Chang discusses within it. The Body Digital marinates with the reader in the way any good novel might, while teaching them something new.
The result is a poetic and well-observed text, which offers the reader a different way of understanding humanity’s relationship with technology. It reminds us that we have coexisted with machines throughout the history of our species, and that they have been helpful and positively shaped the direction of our world. While she covers too much ground to gaze in any one direction for too long, the reader is likely to come away enriched and perhaps even hopeful. And, as Chang points out, we have the opportunity to shape the future of technology, by “attending to the rich, idiosyncratic intelligence of our bodies”.
2025 Melville House Publishing 256pp £14.99 pb / £9.49 ebook
Genuine multipartite entanglement is the strongest form of entanglement, where every part of a quantum system is entangled with every other part. It plays a central role in advanced quantum tasks such as quantum metrology and quantum error correction. To detect this deep form of entanglement in practice, researchers often use entanglement witnesses which are fast, experimentally friendly tests that certify entanglement whenever a measurable quantity exceeds a certain bound.
In this work, the researchers significantly extend previous witness‑construction methods to cover a much broader family of multipartite quantum states. Their approach is built within the multi‑qudit stabiliser formalism, a powerful framework widely used in quantum error correction and known for describing large classes of entangled states, both pure and mixed. They generalise earlier results in two major directions: (i) to systems with arbitrary prime local dimension, going far beyond qubits, and (ii) to stabiliser subspaces, where the stabiliser defines not just a single state but an entire entangled subspace.
This generalisation allows them to construct witnesses tailored to high‑dimensional graph states and to stabiliser‑defined subspaces, and they show that these witnesses can be more robust to noise than those designed for multiqubit systems. In particular, witnesses tailored to GHZ‑type states achieve the strongest resistance to white noise, and in some cases the authors identify the most noise‑robust witness possible within this construction. They also demonstrate that stabiliser‑subspace witnesses can outperform graph‑state witnesses when the local dimension is greater than two.
Overall, this research provides more powerful and flexible tools for detecting genuine multipartite entanglement in noisy, high‑dimensional and computationally relevant quantum systems. It strengthens our ability to certify complex entanglement in real‑world quantum technologies and opens the door to future extensions beyond the stabiliser framework.
Acoustic waves are usually thought of as purely longitudinal, moving back and forth in the direction the wave is travelling and having no intrinsic rotation, therefore no spin (spin‑0). Recent work has shown that acoustic waves can in fact carry local spin‑like behaviour. However, until now, the total spin angular momentum of an acoustic field was believed to vanish, with the local positive and negative spin contributions cancelling each other to give an overall global spin‑0. In this work, the researchers show that acoustic vortex beams can carry a non‑zero longitudinal spin angular momentum when the beam is guided by certain boundary conditions. This overturns the long‑held assumption that longitudinal waves cannot possess a global spin degree of freedom.
Using a self‑consistent theoretical framework, the researchers derive the full spin, orbital and total angular momentum of these beams and reveal a new kind of spin–orbit interaction that appears when the beam is compressed or expanded. They also uncover a detailed relationship between the two competing descriptions of angular momentum in acoustics which are canonical‑Minkowski and kinetic‑Abraham. They demonstrate that only the canonical‑Minkowski form is truly conserved and directly tied to the beam’s azimuthal quantum number, which describes how the wave twists as it travels.
The team further demonstrates this mechanism experimentally using a waveguide with a slowly varying cross‑section. They show that the effect is not limited to this setup, it can also arise in evanescent acoustic fields and even in other wave systems such as electromagnetism. These results introduce a missing fundamental degree of freedom in longitudinal waves, offer new strategies for manipulating acoustic spin and orbital angular momentum, and open the door to future applications in wave‑based devices, underwater communication and particle manipulation.
Quantum-entangled sensors placed over a kilometre apart could allow interferometric measurements of optical light with single photon sensitivity, experiments in the US suggest. While this proof-of-principle demonstration of a theoretical proposal first made in 2012 is not yet practically useful for astronomy, it marks a significant step forward in quantum sensing.
Radio telescopes are often linked together to provide more detailed images with better angular resolution than would otherwise be possible. The Event Horizon Telescope array, for example, performs very long baseline interferometry of signals from observatories on four continents to take astrophysical images such as the first picture of a black hole in 2019. At shorter wavelengths, however, much weaker signals are often parcelled into higher-energy photons. “You start getting this granularity at the single photon level,” says Pieter-Jan Stas at Harvard University.
According to textbook quantum mechanics, one can create an interferometric image from single photons by recombining their paths at a single detector – provided that their paths are not measured before then. This principle is used in laboratory spectroscopy. In astronomical observations, however, attempting to transport single photons from widely spread telescopes to a central detector would almost certainly result in them being lost. The baseline of infrared and optical telescopes is therefore restricted to about 300 m.
In 2012, theorist Daniel Gottesman, then at the Perimeter Institute for Theoretical Physics in Canada, and colleagues proposed using a central single source of entangled photons as a quantum repeater to generate entanglement between two detection sites, putting them into the same quantum state. The effect of an incoming photon on this combined state could therefore be measured without having to recombine the paths and collect the photon at a central detector.
Hidden information
“In reality, the photon will be in a superposition of arriving at both of the detectors,” says Stas. “That’s where this advantage comes from – you have this photon that is delocalized and arrives at both the left and the right station – so you truly have this baseline that helps you with improving your resolution, but to do this you have to keep the ‘which path’ information hidden.”
The 2012 proposal was not thought to be practical, because it required distributing entanglement at a rate comparable with the telescope’s spectral bandwidth. In 2019, however, Harvard’s Mikail Lukin and colleagues proposed integrating a quantum memory into the system. In the new research, they demonstrate this in practice.
The team used qubits made from silicon–vacancy centres in diamond. These can be very long lived because the spin of the centre’s electron (which interacts with the photon) is mapped to the nuclear spin, which is very stable. The researchers used a central laser as a coherent photon source to generate heralded entanglement to certify that the qubits were event-ready. “It’s not like you have to receive the space signal to be simultaneous with the arrival of the photon,” says team member Aziza Suleymanzade at the University of California, Berkeley. “In our case, we distribute entanglement, and it has some coherence time, and during that time you can detect your signal.”
Using two detectors placed in adjacent laboratories and synthetic light sources, the researchers demonstrated photon detection above vacuum fluctuations in fibres over 1.5 km in length. They acknowledge that much work remains before this can be viable in practical astronomy, such as a higher rate of entanglement generation, but Stas says that “this is one step towards bringing quantum techniques into sensing”.
Similar work in China
The research is described in Nature. Researchers in China led by Jian-Wei Pan have achieved a similar result, but their work has yet to be peer reviewed.
Yujie Zhang of the University of Waterloo in Canada points out that Lukin and colleagues have done similar work on distributed quantum communication and the quantum internet. “The major difference is that for most of the original protocols, what people care about is trying to entangle different quantum memories in the quantum network so then they can do gates on those quantum memories,” he says. “There’s nothing about extra information from the environment…This one is different in that they have to get the information mapped from the starlight to their quantum memory.” He notes several difficulties acknowledged by the researchers – such as that vacancy centres are very narrowband, but says that now people know the system can work, they can work to show that it can beat classical systems in practice.
“I think this is definitely a step towards [realizing the protocol envisaged in 2012],” says Gottesman, now at the University of Maryland, College Park. “There have been previous experiments where they generated the entanglement and they did some interference but they didn’t have the repeater aspect, which is the real value-added aspect of doing quantum-assisted interferometry. Its rate is still well short of what you’d need to have a functioning telescope, but this is putting one of the important pieces into place.”
The heads of university physics departments in the UK have published an open letter expressing their “deep concern” about funding changes announced late last year by UK Research and Innovation (UKRI), the umbrella organization for the UK’s research councils.
Addressed to science minister Patrick Vallance, the letter says the cuts are causing “reputational risk” and calls for “strategic clarity and stability” to ensure that UK physics can thrive.
It has so far been signed by 58 people who represent 45 different universities, including Birmingham, Bristol, Cambridge, Durham, Imperial College, Liverpool, Manchester and Oxford.
The letter says that the changes at UKRI “risk undermining science’s fundamental role in improving our prosperity, health and quality of life, as well as delivering sustainable growth through innovation, productivity and scientific leadership”.
The signatories warn that the UK’s international standing in physics is “a strategic asset” and that areas such as particle physics, astronomy and nuclear physics are “especially important”.
Raising concerns
The decision by the heads of physics to write to Vallance comes in the wake of UKRI stating in December that it will be adjusting how it allocates government funding for scientific research and infrastructure.
The Science and Technology Facilities Council (STFC), which is part of UKRI, stated that projects would need to be cut given inflation, rising energy costs as well as “unfavourable movements in foreign exchange rates” that have increased STFC’s annual costs by over £50m a year.
The STFC noted that it would need to reduce spending from its core budget by at least 30% over 2024/2025 levelswhile also cutting the number of projects financed by its infrastructure fund.
The council has already said two UK national facilities – the Relativistic Ultrafast Electron Diffraction and Imaging facility and a mass spectrometry centre dubbed C‑MASS – will now not be prioritized.
In addition, two international particle-physics projects will not be supported: a UK-led upgrade to the LHCb experiment at CERN as well as a contribution to the Electron-Ion Collider at the Brookhaven National Laboratory that is currently being built.
Philip Burrows, director of the John Adams Institute for Accelerator Science at the University of Oxford, who is one of the signatories of the letter, told Physics World that the cuts are “like buying a Formula-1 car but not being able to afford the driver”.
Burrows admits that the STFC has been hit “particularly hard” by its flat-cash settlement, given that a large fraction of its expenditure pays the UK’s subscriptions to international facilities and operating the UK’s flagship national facilities.
But because most of the rest of the STFC’s budget supports scientists to do research at those facilities, he is concerned that the funding cuts will fall disproportionately on the science programme.
“Constraining these areas risks weakening the very talent pipeline on which the UK’s innovation economy depends,” the letter states. “Fundamental physics also delivers substantial public engagement and cultural impact, strengthening public support for science and reinforcing the UK’s reputation as a global scientific leader.”
The signatories also say they are “particularly concerned” about the UK’s capacity to lead the scientific exploitation of major international projects. “An abrupt pause in funding for key international science programmes risks damaging UK researchers’ competitive advantage into the 2040s,” they note.
The letter now calls on the government to work with UKRI and STFC to “stabilize” curiosity-driven grants for physics within STFC “at a minimum of flat funding in real terms” as well as protect postdocs, students and technicians from the cuts.
It also calls on the UK to develop a long-term strategy for infrastructure and call on the government to address facilities cost pressures through “dedicated and equitable mechanisms so that external shocks do not singularly erode the UK’s research base in STFC-funded research areas”.
The news comes as Michele Dougherty today formally stepped down from her role as IOP president. Dougherty, who also holds the position of executive chair of the STFC, had previously stepped back from presidential duties on 26 January due to a conflict of interest.
Paul Howarth, who has been IOP president-elect since September, will now become IOP president.
The Earth’s magnetic poles have reversed 540 times over the past 170 million years. Usually, these reversals are relatively speedy in geological terms, taking around 10,000 years to complete. Now, however, scientists in the US, France and Japan have found evidence of much slower reversals deep in Earth’s geophysical past. Their findings could have important implications for our understanding of Earth’s climate and evolutionary history.
Scientists think the Earth’s magnetic field arises from a dynamo effect created by molten metal circulating inside the planet’s outer core. Its consequences include the bubble-like magnetosphere, which shields us from the solar wind and cosmic radiation that would otherwise erode our atmosphere.
From time to time, this field weakens, and the Earth’s magnetic north and south poles switch places. This is known as a geomagnetic reversal, and we know about it because certain types of terrestrial rocks and marine sediment cores contain evidence of past reversals. Judging from this evidence, reversals usually take a few thousand years, during which time the poles drift before settling again on opposite sides of the globe.
Looking into the past
Researchers led by Yuhji Yamamoto of Kochi University, Japan and Peter Lippert at the University of Utah, US, have now identified two major exceptions to this rule. Drawing on evidence obtained during the Integrated Ocean Drilling Program expedition in 2012, they say that around 40 million years ago, during the Eocene epoch, the Earth experienced two reversals that took 18,000 and 70,000 years.
The team based these findings on cores of sediment extracted off the coast of Newfoundland, Canada, up to 250 metres below the seabed. These cores contain crystals of magnetite that were produced by a combination of ancient microorganisms and other natural processes. The iron oxide particles within these crystals align with the polarity of the Earth’s magnetic field at the time the sediments were deposited. Because marine sediments are far less affected by erosion and weathering than sediments onshore, Yamamoto says the information they preserve about past Earth environments – including geomagnetic conditions – is exceptionally clean.
Significance for evolutionary history
The team says the difference between a geomagnetic reversal that takes 10,000 years and one that takes 70,000 years is significant because prolonged intervals of weaker geomagnetic fields would have exposed the Earth to higher amounts of cosmic radiation for longer. The effects on living creatures could have been devastating, says Lippert. As well as higher rates of genetic mutations due to increased radiation, he points out that organisms from bacteria to birds use the Earth’s magnetic field while navigating. “A lower strength field would create sustained pressures on these organisms to adapt,” he says.
If humans had existed at the time of these reversals, the effects on our species could have been similarly profound. “Modern humans (Homo sapiens) are thought to have begun dispersing out of Africa only about 50,000 years ago,” Yamamoto observes. “If a geomagnetic reversal can persist for a period comparable to – or even longer than – this timescale, it implies that the Earth’s environment could undergo substantial and continuous change throughout the entire period of human evolution.”
Although our genetic ancestors dodged that particular bullet, Yamamoto thinks the team’s findings, which are published in Nature Communications Earth & Environment, offer a valuable perspective on how evolution and environmental change could interact in the future. “This period corresponds to an epoch when Earth was far warmer than it is today, and when Greenland is thought to have been a truly ‘green land’,” he explains. “We also know that atmospheric CO₂ concentrations during this era were comparable to levels projected for the end of this century, making it an important ‘climate analogue’ for understanding near‑future climate conditions.”
The discovery could also have more direct implications for future life on Earth. The magnitude of the Earth’s magnetic field has decreased by around 5% in each century since records began. This decrease, combined with the slow drift of our current magnetic North Poletowards Siberia, could indicate that we are in the early stages of a new geomagnetic reversal. Re‑evaluating the duration of such reversals is thus not only an issue for geophysicists, Yamamoto says. It’s also an important opportunity to reconsider fundamental questions about how we should coexist with our planet and how we ought to confront a continually changing environment.
Motivation for future studies
John Tarduno, a geophysicist at the University of Rochester, US, who was not involved in the study, describes it as “outstanding” work that “documents an exciting discovery bearing on the nature of magnetic shielding through time and the geomagnetic reversal process”. He agrees that reduced shielding could have had biotic effects, and adds that the discovery of long reversal transitions could influence scientific thinking on the statistics of field reversals – including questions of whether the field retains some “memory” of previous events. “This new study will provide motivation to examine reversal transitions at very high resolution,” Tarduno says.
For their next project, Yamamoto and colleagues aim to use sequences of lava flows in Iceland to analyse how the Earth’s magnetic field evolved. Lippert’s team, for its part, will be studying features called geomagnetic excursions that appear in both deep sea and terrestrial sediments. Such excursions are evidence of short-lived, incomplete attempts at field reversals, and Lippert explains that they can be excellent stratigraphic markers, helping scientists correlate records on geological timescales and compare them with samples taken from different parts of the world. “Excursions, like long reversals, can inform our understanding of what ultimately causes a geomagnetic field reversal to start and persist to completion,” he says.
Fusion adopter Debbie Callahan is chief strategy officer at Focused Energy. (Courtesy: Focused Energy)
With the world’s energy demands increasing, and our impact on the climate becoming ever clearer, the search is on for greener, cleaner energy production. That’s why research into fusion energy is undergoing something of a renaissance.
Construction of the International Thermonuclear Experimental Reactor (ITER) in France – the world’s largest fusion experiment – is currently under way, while there are numerous other large-scale facilities and academic research projects too. There has also been a rise in the number of smaller commercial companies joining the race.
One person at the forefront of fusion research is Debbie Callahan – a plasma physicist who spent 35 years working at the National Ignition Facility (NIF) at Lawrence Livermore National Laboratory in the US. She is now chief strategy officer at Focused Energy, a laser-fusion firm based in Germany and California, which is trying to generate energy from the laser-driven fusion of hydrogen isotopes.
Callahan recently talked to Physics World online editor Hamish Johnston about working in the fusion sector, Focused Energy’s research and technology, and the career opportunities available. The following is an edited extract of their conversation, which you can hear in full on the Physics World Weekly podcast.
How does NIF’s approach to fusion differ from that taken by magnetic confinement facilities such as ITER?
To get fusion to happen, you need three elements that we sometimes call the triple product. You need a certain amount of density in your plasma, you need temperature, and you need time. The product of those has to be over a certain value.
Magnetic fusion and inertial fusion are kind of the opposite of each other. In a magnetic fusion system like ITER, you have a low-density plasma, but you hold it for a long time. You do that by using magnetic fields that trap the plasma and keep it from escaping.
In inertial fusion – like at NIF – it’s the opposite. You don’t hold the plasma together at all, it’s only held by its own inertia, and you have a very high density for a short time. In both cases, you can make fusion happen.
What is the current state of the art at NIF, in terms of how much energy you have to put in to achieve fusion versus how much you get out?
To date, the best shot at NIF – by which I mean an individual, high-energy laser bombardment of the target capsule – occurred during an experiment in April 2025, which had a target gain of about 4.1. That means that they got out 4.1 times the amount of energy that they put in. The incident laser energy for those shots is around two megajoules, so they got out about eight megajoules.
This is a tremendous accomplishment that’s taken decades to get to. But to make inertial fusion energy successful and use it in a power plant, we need significantly higher gains of more like 50 to 100.
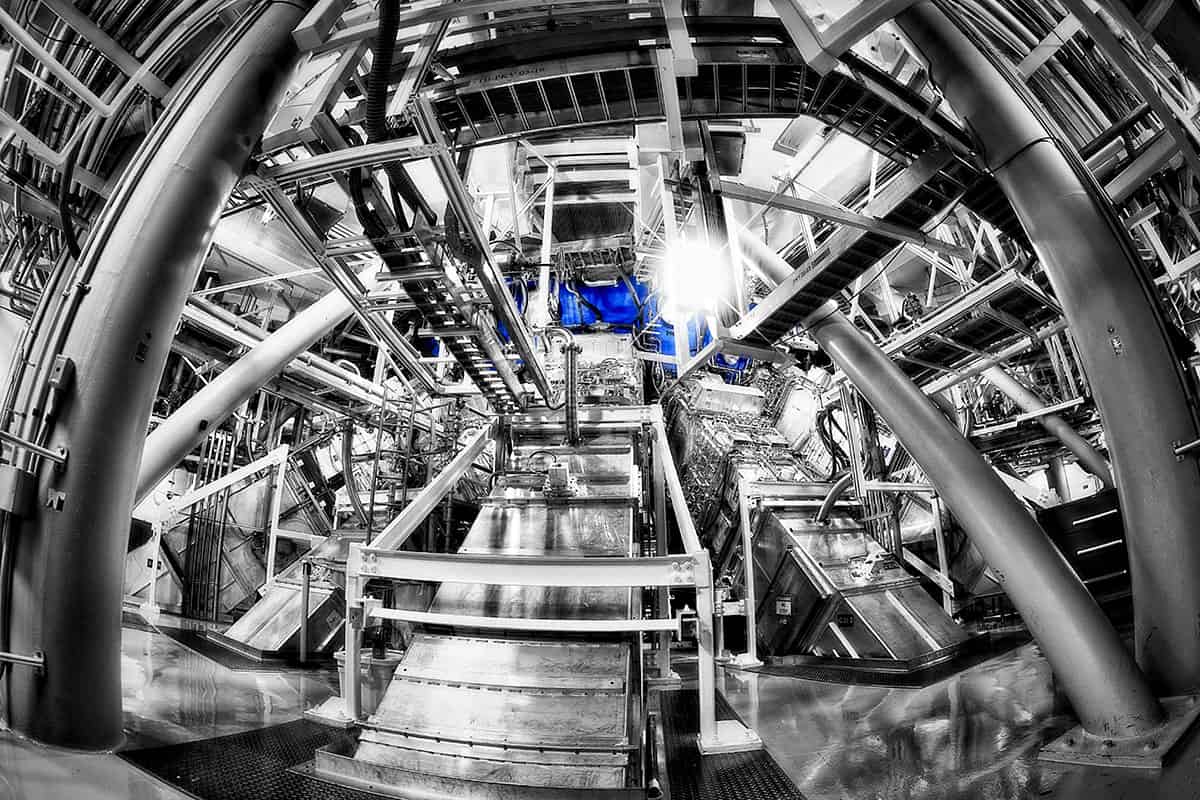
Captured beams The target chamber of the National Ignition Facility (NIF) at Lawrence Livermore National Laboratory. NIF has demonstrated that inertial fusion can work with deuterium–tritium fuel, but it is a research facility not a commercial endeavour. (Courtesy: Lawrence Livermore National Laboratory/Damien Jemison)
Can you explain Focused Energy’s approach to fusion?
Focused Energy was founded in July 2021, and has offices in the US and Germany. Just a month later, we achieved fusion ignition, which is when the fusion fuel becomes hot enough for the reactions to sustain themselves through their own internal heating (it is not the same as gain).
At NIF lasers are fired into a small cylinder of gold or depleted uranium and the energy is converted into X-rays, which then drive the capsule. It’s what’s called laser indirect drive. At Focused Energy, however, we’re directly driving the capsule. The laser energy is put directly on the capsule, with no intermediate X-rays.
The advantage of this approach is that converting laser energy to X-rays is not very efficient. It makes it much harder to get the high target gains that we need. At Focused Energy, we believe that direct drive is the best option for fusion energy to get us to a gain of over 50.
So is boosting efficiency one of your key goals to make fusion practical at an industrial level?
Yes, exactly. You have to remember that NIF was funded for national security purposes, not for fusion energy. It wasn’t designed to be a power plant – the goal was just to generate fusion energy for the first time.
In particular, the laser at NIF is less than 1% efficient but we believe that for fusion power generation, the laser needs to be about 10% efficient.
So one of the big thrusts for our company is to develop more efficient lasers that are driven by diodes – called diode pump solid state lasers.
Can you tell us about Focused Energy’s two technologies called LightHouse and Pearl Fuel?
LightHouse is our fusion pilot plant. When operational, it will be the first power plant to produce engineering gain greater than one, meaning it will produce more energy than it took to drive it. In other words, we’ll be producing net electricity.
For NIF, in contrast, gain is the amount of energy out relative to the amount of laser energy in. But the laser is very inefficient, so the amount of electricity they had to put in to produce that eight megajoules of fusion energy is a lot.
Meanwhile, Pearl is the capsule the laser is aimed at in our direct drive system. It’s filled with deuterium–tritium fuel derived from sea water and lithium.
Rejuvenating nuclear A rendering of Focused Energy’s proposed fusion power plant at the Biblis fission power plant in Germany, which was shut down in 2011. (Courtesy: Focused Energy)
How do you develop the capsule to absorb the laser energy and give as much of it to the fuel as possible?
The development of the capsule for a fusion power plant is quite complicated. First, we need it to be a perfect sphere so it compresses spherically. The materials also need to efficiently absorb the laser light so you can minimize the size of that laser.
You have to be able to cheaply and quickly mass produce these targets too. While NIF does 400 shots per year, we will need to do about 900,000 shots a day – about 10 per second. We’ll also have to efficiently remove the exploded target material from the reactor chamber so that it can be cleared for the next shot.
It’s a very complicated design that needs to bring together all the pieces of the power plant in a consistent way.
When you are designing these elements, what plays a bigger role – computer simulations or experiments?
Computer simulations play a large part in developing these designs. But one of the lessons that I learned from NIF was that, although the simulation codes are state of the art, you need very precise answers, and the codes are not quite good enough – experimental data play a huge role in optimizing the design. I expect the same will be true at Focused Energy.
A third factor that’s developing is artificial intelligence (AI) and machine learning. In fact, at Livermore, a project working on AI contributed to achieving gain for the first time in December 2022. I only see AI’s role in fusion getting bigger, especially once we are able to do higher repetition rate experiments, which will provide more training data.
What intellectual property (IP) does Focused Energy have in addition to that for the design of the Pearl target and the LightHouse plant?
We also have IP in the design of the lasers – they are not the same lasers as used at NIF. And I think there’ll be a lot of IP around how we fabricate the targets. After all, it’s pretty complicated to figure out how to build 900,000 targets a day at a reasonable cost.
We’ll see a lot of IP coming out of this project in those areas, but there’s also the act of putting it all together. How we integrate these things in order to make a successful plant is important.
What are the challenges of working with deuterium and tritium as materials for fusion?
We chose deuterium and tritium because they are the easiest elements to fuse, and have been successfully demonstrated as fusion fuel by NIF.
Deuterium can be found naturally in sea water, but getting tritium – which is radioactive – is more complicated. We breed it from lithium. Our reactor designs have lithium in them, and the neutrons from the fusion reactions breed the tritium.
Making sure that we have enough tritium, and figuring out how to extract that material to use it for future shots, is a big task. We have to be able to breed enough tritium to keep the plant going.
To work on this, we have a collaboration funded by the US Department of Energy to work with Savannah River National Lab in South Carolina. They have a lot of expertise in designing these tritium-extraction systems.
How will you capture the heat from the deuterium–tritium fusion reaction?
We will use a conventional steam cycle to convert the heat into electricity. It’s funny – we’ll have this very hi-tech way of producing heat, but at the end of the day, we will use a traditional system to produce the electricity from that heat.
So what’s the timeline on development?
Our plan is to have a pilot plant up by the end of the 2030s. It’s a fairly aggressive timeline given the things that we have to do. But that’s part of being a start-up – we have to take some risks and try to move quickly to achieve our goal.
To help that we have, in my view, a superpower – we have one foot in Europe and one foot in the US. There are a lot of opportunities between the two continents to partner with other companies, universities and governments. I think that makes us strong because we have access to some of the best talent from around the world.
How does working at Focused Energy compare with life as an academic at Lawrence Livermore?
There are a lot of similarities. My role now is to bring the knowledge and skills I learned at NIF to Focused Energy, so it’s been a natural transition.
In fact, there was a lot of pressure working at NIF. We were trying to move very quickly, so it’s actually very similar to working in a start-up like Focused Energy.
One of the big differences is the level of bureaucracy. Working for a government-funded lab meant there were lots of rules and paperwork, which takes up your time and you don’t always see the value in it.
In contrast, working for a small start-up means we can move more quickly because we don’t have as many of those kinds of constraints. Personally, I find that great because it leaves more time for the fun and interesting things – like trying to get fusion on the grid.
Are you still involved in academic research in any way?
As a firm, we are still out there collaborating with academics. Last year, for example, we gave four separate presentations at the American Physical Society Division of Plasma Physics meeting.
Active collaboration Debbie Callahan presenting the work of Focused Energy at the IEEE Pulsed Power and Plasma Science Conference in Berlin in June 2025. (Courtesy: Focused Energy)
I feel very strongly about peer review. Of course, publishing isn’t our number one priority, but we need feedback from others. We’re trying to do something that no-one’s done before, so it’s important to have our colleagues give us feedback on what we’re doing, point out mistakes we’re making or things we’re forgetting.
Working with universities and national labs in both Europe and the US is vital. Communicating with others in the field is important for us to get to where we want to go.
And of course, being an active part of the fusion community is good for recruitment too. We regularly give presentations at conferences that students attend. We meet those students and they learn about our work – and they might be future employees for our company.
What’s your advice for early-career physicists keen on joining the fusion industry?
There are so many opportunities right now, especially compared to the start of my career when the work was mainly just at universities or national labs. Nowadays, there are a lot of companies in the sector. Not all of them will survive because there’s only so much money, but there are still lots of opportunities. If you’re interested in fusion energy, go for it.
The field is always developing. There’s new stuff happening every day – and new problems. So if you like problem-solving, it’s great, especially if you want to do something good for the world.
There are also opportunities for people who are not plasma physicists. At Focused Energy we have people across so many fields – those who work on lasers, others who work on reactor design, some developing the AI and machine learning, and those who work on target physics, like me. To achieve fusion energy, we need physicists, engineers, mathematicians and computer scientists. We need researchers, technicians and operators. There’s going to be tremendous growth in this sector.
This winter in Bristol has been even gloomier than usual – so I was really looking forward to the Bristol Light Festival 2026. We went on the last evening of the event (28 February) and we were blessed with dry weather and warmish temperatures.
The festival featured 10 illuminated installations that were scattered throughout Bristol and the crowds were out in force to enjoy them. I wasn’t expecting to be thinking about physics as I wandered through town, but that’s exactly what I found myself doing at an installation called The Midnight Ballet by the British sculptor Will Budgett. Rather appropriately, it was located next to the HH Wills Physics Laboratory at the University of Bristol.
The display comprises seven sculptures that are illuminated from two different directions. The result is two very different images of ballerinas projected onto two screens (see image).
Art and science
So, why was I thinking about physics while admiring the work? To me the pieces embody – in a purely artistic way – the idea of superposition and measurement in quantum mechanics. A sculpture is capable of producing two different images (a superposition of states), but neither of these images is observable until a sculpture is illuminated from specific directions (the measurements).
Now, I know that this analogy is far from perfect. Measurements can be made simultaneously in two orthogonal planes, for example. But, Budgett’s beautiful artworks really made me think about quantum physics. Given the exhibit’s close proximity to the university’s physics department, I suspect I am not the only one.
In 1942 physicists in Chicago, led by Enrico Fermi, famously produced the world’s first self-sustaining nuclear chain reaction. But it was to be another nine years before electricity was generated from fission for the first time. That landmark event occurred in 1951 when the Experimental Breeder Reactor-I in southern Idaho powered a string of four 200-watt light bulbs.
Our ability to harness nuclear power has been under constant development since then. In fact, according to the Nuclear Energy Association, a record 2667 terrawatt-hours of electricity was generated by nuclear reactors around the world in 2024 – up 2.5% on the year before. But what, I wonder, is the potential of nuclear-powered transport?
A “nuclear engine” has many advantages, notably providing a vehicle with an almost unlimited supply of onboard power, with no need for regular refuelling. That’s particularly attractive for large ships and submarines, where fuel stops at sea are few and far between. It’s even better for space craft, which cannot refuel at all.
The downside is that a vehicle needs to be fairly large to carry even a small nuclear fission reactor – plus all the heavy shielding to protect passengers onboard. Stringent safety requirements also have to be met. If the vehicle were to crash or explode, the shield around the reactor needs to stay fully intact.
Ships and planes
Perhaps the best known transport application of nuclear power is at sea, where it’s used for warships, submarines and supercarriers. The world’s first nuclear-powered ship was the US Navy submarine Nautilus, which was launched in 1954. As the first vessel to have a nuclear reactor for propulsion, it revolutionized naval capabilities.
Compared to oil or coal-fired ships, nuclear-powered vessels can travel far greater distances. All the fuel is in the reactor, which means there is no need for additional fuel be carried onboard – or for exhaust chimneys or air intakes. Even better, the fuel is relatively cheap. But operating and infrastructure costs are steep, which is why almost all nuclear-powered marine vessels belong to the military.
There have, however, been numerous attempts to develop other forms of nuclear-powered transport. While a nuclear-powered aircraft might seem unlikely, the idea of flying non-stop to the other side of the world, without giving off any greenhouse-gas emissions, is appealing. Incredible as it might seem, airborne nuclear reactors were actually trialled in the mid-1950s.
That was when the United States Air Force converted a B-36 bomber to carry an operational air-cooled reactor, weighing around 18 tons. The aircraft was not actually nuclear powered but it was operated in this configuration to assess the feasibility of flying a nuclear reactor. The aircraft made a total of 47 flights between July 1955 and March 1957.
In 1955, the Soviet Union also ran a project to adapt a Tupolev Tu-95 “Bear” aircraft for nuclear power. However, because of the radiation hazard to the crew and the difficulties in providing adequate shielding, the project was soon abandoned. Neither the American or the Soviet atomic-powered aircraft ever flew and – because the technology was inherently dangerous – it was never considered for commercial aviation.
Cars and trains
The same fate befell nuclear-powered trains. In 1954 the US nuclear physicist Lyle Borst, then at the University of Utah, proposed a 360-tonne locomotive carrying a uranium-235 fuelled nuclear reactor. Several other countries, including Germany, Russia and the UK, also had schemes for nuclear locos. But public concerns about safety could not be overcome and nuclear trains were never built. The $1.2m price tag of Borst’s train didn’t help either.
Nuclear nightmare Ford’s Nucleon car thankfully never got past the concept stage.
In the late 1950s, meanwhile, there were at least four theoretical nuclear-powered “concept cars”: the Ford Nucleon, the Studebaker Packard Astral, the Simca Fulgur and the Arbel Symétric. Based on the assumption that nuclear reactors would get much smaller over time, it was felt that such a car would need relatively light radiation shielding. I certainly wouldn’t have wanted to take one of those for a spin; in the end none got beyond concept stage.
Perhaps the real success story of nuclear propulsion has been in space.
But perhaps the real success story of nuclear propulsion has been in space. Between 1967 and 1988, the Soviet Union pioneered the use of fission reactors for powering surveillance satellites, with over 30 nuclear-powered satellites being launched during that period. And since the early 1960s, radioisotopes have been a key source of energy in space.
Driven by the desire for faster, more capable and longer duration space missions to the Moon, Mars and beyond, China, Russia and the US are now investing significantly in the next generation of nuclear reactor technology for space propulsion, where solar or radioisotope power will be inadequate. Several options are on the table.
One is nuclear thermal propulsion, whereby energy from a fission reactor heats a propellant fuel. Another is nuclear electric propulsion, in which the fission energy ionizes a gas that gets propelled out the back of the spacecraft. Both involve using tiny nuclear reactors of the kind used in submarines, except they’re cooled by gas, not water. Key programmes are aiming for in-space demonstrations in the next 5–10 years.
Where next?
Many of the first ideas for nuclear-powered transport were dreamed up little more than a decade after the first self-sustaining chain reaction. The appeal was clear: compared to other fuels, nuclear power has a high energy density and lasts much longer. It also has zero carbon emissions. Nuclear power must have seemed a panacea for all our energy needs – using it for cars and planes must have seen an obvious next step.
However, there are major safety issues to address when nuclear sources are mobilized, from protecting passengers and crew, to ensuring appropriate safeguards should anything go wrong. And today we understand all too well the legacy of nuclear systems, from the safe disposal of spent fuel to the decommissioning of nuclear infrastructure and equipment.
We’ve struck the right balance when it comes to using nuclear power, confining it to sea-faring vessels under the watchful eye of the military.
Here on Earth, I think we’ve struck the right balance when it comes to using nuclear power, confining it to sea-faring vessels under the watchful eye of the military. But as human-crewed, deep-space exploration beckons, a whole new set of issues will arise. There will, of course, be lots of technical and engineering challenges.
How, for example, will we maintain, repair and decommission nuclear-powered space craft? How will we avoid endangering crews or polluting the environment especially when craft take off? Who should set appropriate legislation – and how we do we police those rules? When it comes to space, nuclear will help us “to boldly go”; but it will also require bold regulation.
Congratulations on winning the 2025 JPhys Materials Early Career Award. What does this mean for you at this stage of your career?
I am really grateful to the Editorial Board of JPhys Materials for this award and for highlighting our work. This is a key recognition for the whole team behind the results presented in this research paper. We were taking a new turn in our research with this topic – trying to convince bubbles to assemble into crystalline structures towards architected materials – and this award is an important encouragement to continue pushing in this direction. At the crossroads of physics, physical chemistry, materials science and mechanics, we hope that this is only the beginning of our interdisciplinary journey around bubble assemblies and foam-based materials.
Your research explores elasto-capillarity and foam architectures, what inspired you to work in this fascinating area?
I always say that research is a series of encounters – with people, and with scientific themes and objects. I was lucky to discover this interdisciplinary world as an undergraduate, during an internship on elasto-capillarity at the intersection of physics and mechanics. The scientific communities working on these topics – and also on foams – are fantastic. In both fields, I was fortunate to meet talented people who inspired my future work, combining scientific skills and creativity.
In France, the GDR MePhy (mechanics and physics of complex systems) played a key role in broadening my perspective, by organizing workshops on many different topics, always with interdisciplinarity in mind.
You have demonstrated mechanically guided self-assembly of bubbles leading to crystalline foam structures. What’s the significance of this finding and how could it impact materials design?
In the paper, part of the journal’s Emerging Leaders collection, we provide a proof-of-concept with alginate and polyurethane materials to demonstrate that it is possible to use a fibre array to order bubbles into a crystalline structure, which can be tuned by choosing the fibre pattern, and to keep this ordering upon solidification to provide an alternative approach to additive manufacturing. This work is mainly fundamental, and we hope it paves the way toward a wider use of mechanical self-assembly principles in the context of porous architected materials.
The use of solidifying materials for those studies is two-fold: first, it allows us to observe the systems with X-ray microtomography once solidified, and second, it demonstrates that we could use such techniques to build actual solid materials.
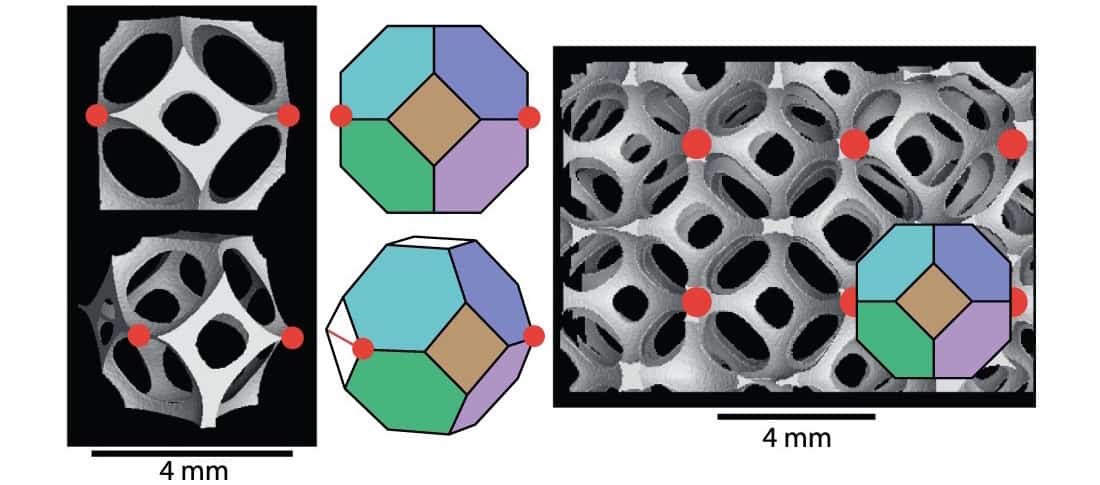
Guiding bubbles with fibre arrays Arrangements of bubbles constrained by a network of fibres (highlighted with red dots) can exhibit long-range order and even include Kelvin cell arrangements. (Courtesy: J. Phys. Mater. 10.1088/2515-7639/adaa21)
What excites you most about this field right now, and where do you see the biggest opportunities for breakthroughs?
Combining physical understanding and materials science is certainly a great area of opportunity to better exploit mechanical self-assembly. It is very compelling to search for strategies based on physical principles to generate materials with non-trivial mechanical or acoustic properties. Capillarity, elasticity, stimuli-induced modification of systems, as well as geometrical considerations, all offer a great playground to explore. Curiosity-driven research has many advantages, and often, unexpected observations completely reshape the trajectory that we had in mind.
Could you tell us about your team’s current research priorities and the directions you are most focused on?
We believe that focusing first on the underlying physical principles, especially in terms of mechanical self-assembly, will provide the building blocks to generate novel materials. One key research axis we are exploring now is widening the range of materials that can be used for “liquid foam templating” (a general approach that involves controlling the properties of a foam in its liquid state to control the resulting properties of the foam after solidification). We focus on the solidification mechanisms, either by playing with external stimuli or by controlling the solidification reactions via the introduction of catalysts or solidifying agents.
What are the key challenges in achieving ordered structures during solidification?
Liquid foams provide beautiful hierarchical structures that are also short-lived. To take advantage of the mechanical self-assembly of bubbles to build solid materials, understanding the relevant timescales is key: depending on whether the foam has time to drain and destabilize before solidification or not, its final morphology can be completely different. Controlling both the ageing mechanisms and the solidification of the matrix is particularly challenging.
How do you see foam-based materials impacting real-world applications?
Both biomedical devices and soft robots often rely on soft materials – either to match the mechanical properties of biological tissues or to provide the mechanical properties to build soft robots to enable motion. Being able to customize self-assembled hierarchical structures could allow us to explore a wider range of even softer materials, with specific properties resulting from their structural features. Applications could also extend to stiffer materials, mainly in the context of acoustic properties and wave propagation in such architected structures.
What are the most surprising behaviours you have observed during the processes of self-assembly and solidification of foams?
For the experiments detailed in the paper, the structures revealed their beauty once the X-ray tomography scans were performed. When we varied the parameters, we could only guess what was going to happen before getting the visual confirmation a few hours later. We were really happy to see that changing the pattern of the fibre array could indeed provide different ordered foam structures. In some other projects we are working on, foam stability has been a real challenge. We were sometimes surprised to obtain long-lasting liquid systems.
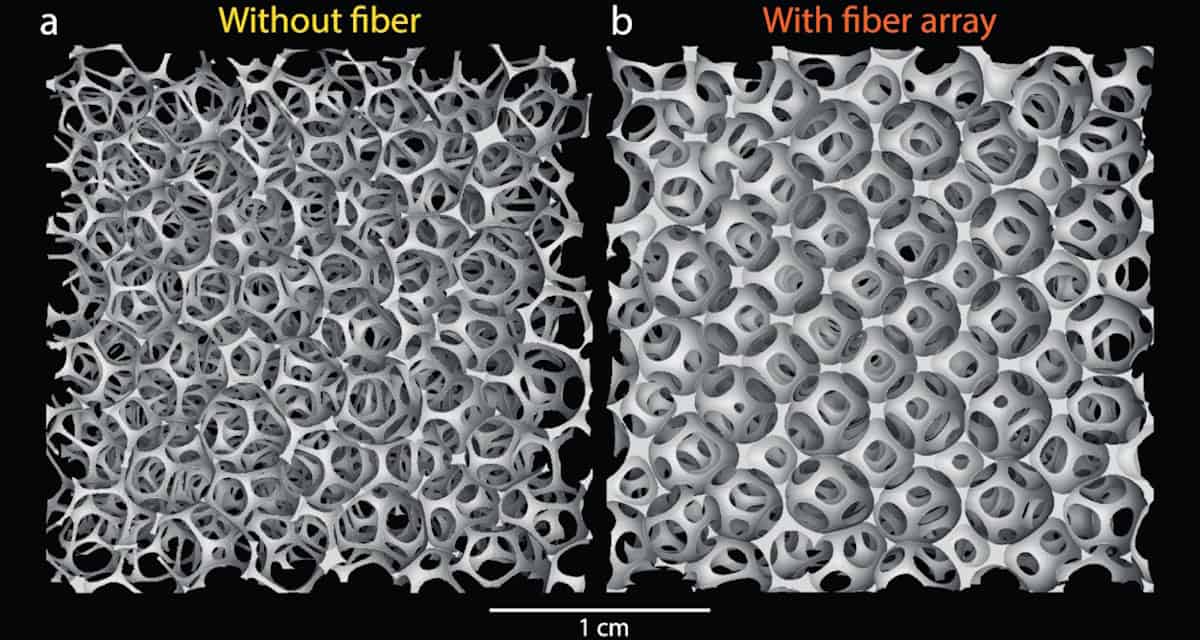
Creating order X-ray tomography scans of foams without a fibre array (left), showing a disordered structure, and with a square fibre array (right), showing large ordered zones. (Courtesy: J. Phys. Mater. 10.1088/2515-7639/adaa21)
Looking ahead, what are the next big questions you hope to tackle in your field?
In the fundamental context of the physics and mechanics of elasto-capillarity, the study of model systems involving self-assembly mechanisms will be a key aspect of our research. I then hope to successfully identify key applications for such architected systems – mainly in the fields of mechanical or acoustic metamaterials, but also for biomedical engineering. Regarding foam solidification, understanding the mechanisms of pore opening during the solidification process – leading to either closed-cell or open-cell foams – is also an important question for the community.
That fantastic experience allowed me to work in a group with numerous people from many different backgrounds, pushing the frontiers of interdisciplinarity in ways I could not have imagined before joining the Rogers group as a postdoc. At the moment, I am focusing on more fundamental questions, but it is definitely important to keep in mind what physics and materials science can bring to a broad variety of applications that offer solutions for society, in biomedical engineering and beyond.
Your research often combines theory and experiment and involves interdisciplinary collaboration. How do you see these collaborations shaping the future of your field?
It is always the scientific questions we want to answer – or the goals we aim to achieve – that should define the collaborations, bringing together multiple skills and backgrounds to tackle a shared challenge. Clearly, at the intersection of physics, physical chemistry, materials science and mechanics, there are many interesting questions that require contributions from different disciplines and skillsets. A key aspect is how people trained in different areas learn to “speak the same language” in order to advance interdisciplinary topics.
3D structural analysis The team’s foam research projects make extensive use of X-ray microtomography on the MINAMEC platform at Institut Charles Sadron. (Courtesy: Aurélie Hourlier-Fargette)
How do you envision your research evolving over the next 5–10 years?
I hope to be able to combine fundamental research and meaningful applications successfully – perhaps in the form of medical devices or tools for soft robots. There are many exciting possibilities, but it is certainly still too early for me to predict.
What advice would you give early-career researchers pursuing interdisciplinary projects?
Believe in what you are doing! We push boundaries more easily in areas we are passionate about, and we are also more productive when we work on topics for which we have found a supportive environment – with a unique combination of collaborators and access to state-of-the-art equipment.
In research, and especially in interdisciplinary fields, a key challenge is finding the right balance: you need to stay focused on the research projects that matter for you, while also keeping an open mind and staying aware of what others are doing. This broader vision helps you understand how your work integrates into a larger, more complex landscape.
Finally, what inspires you most as a scientist, and what keeps you motivated during challenging phases of research?
I have always liked working with desktop-scale experiments, where we can touch the objects and have an intuition for the physical mechanisms behind the observed phenomena.
Another source of inspiration is the beauty of the scientific objects that we study. With droplets, bubbles and foams – which are not only scientifically interesting but also beautiful – there is a strong connection with art and photography.
And finally, a key aspect of our professional life is the people we work with. It is clearly an additional motivation to feel part of a community where we can discuss both scientific questions and ways to improve how research is organized, as well as help younger students, PhDs and postdocs find their professional path. Working with amazing colleagues definitely helps when the path is longer or more difficult than expected.
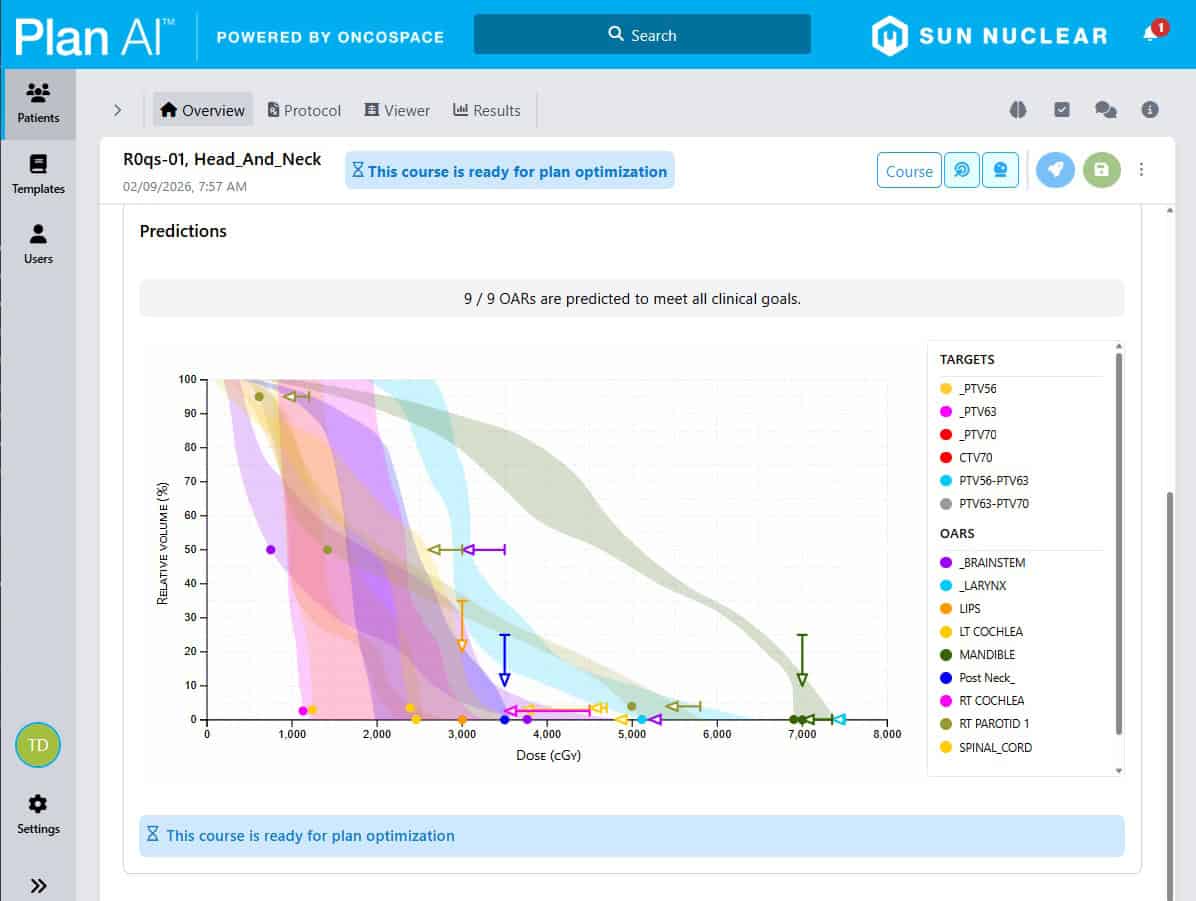
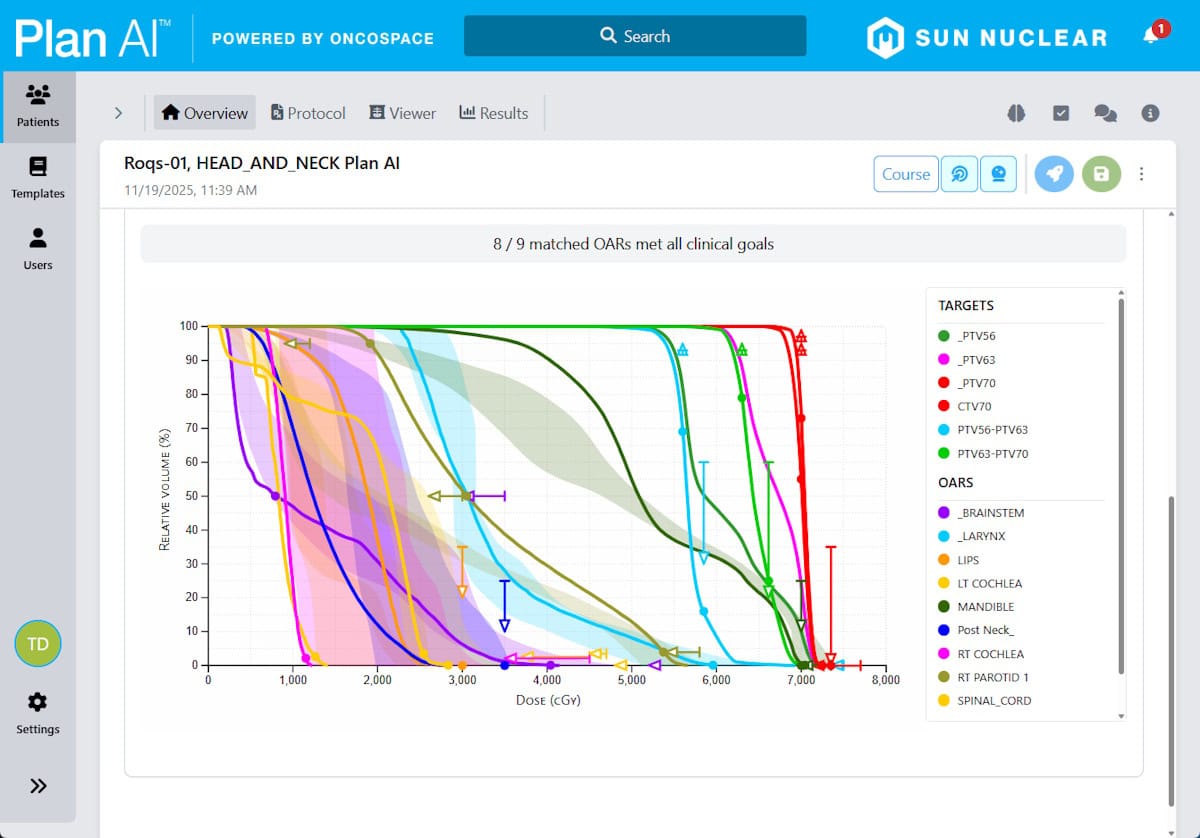
This webinar explores how smart shielding is transforming the design of Leksell Gamma Knife radiosurgery environments, shifting from bunker‑like spaces to open, patient‑centric treatment rooms. Drawing from dose‑rate maps, room‑dimension considerations and modern shielding innovations, we’ll demonstrate how treatment rooms can safely incorporate features such as windows and natural light, improving both functionality and patient experience.
Dr Riccardo Bevilacqua will walk through the key questions that clinicians, planners and hospital administrators should ask when evaluating new builds or upgrading existing treatment rooms. We will highlight how modern shielding approaches expand design possibilities, debunk outdated assumptions and offer practical guidance on evaluating sites and educating stakeholders on what lies “beyond bunkers”.
Dr Riccardo Bevilacqua
Dr Riccardo Bevilacqua, a nuclear physicist with a PhD in neutron data for Generation IV nuclear reactors from Uppsala University, has worked as a scientist for the European Commission and at various international research facilities. His career has transitioned from research to radiation safety and back to medical physics, the field that first interested him as a student in Italy. Based in Stockholm, Sweden, he leads global radiation‑safety initiatives at Elekta. Outside of work, Riccardo is a father, a stepfather and writes popular‑science articles on physics and radiation.
If you have ever watched a basketball match, you will know that along with the sound of the ball being bounced, there is also the constant squeaking of shoes as the players move across the court.
Such noise is a common occurrence in everyday life from the scraping of chalk on a blackboard to when brakes are applied on a bicycle.
Physicists in France, Isreal, the UK and the US have now recreated the phenomenon in a lab and discovered that the squeaking is due to a previously unseen mechanism.
Previous studies looking at the effect suggested that “pulses” are created when two materials “stick and slip”, but such studies focused on slow movements, which do not create squeaks.
The team instead found that the noise was not caused by random stick-slip events, but rather deformations of the rubber sole pulsing in bursts, or rippling,across the surface.
In this case, small parts of the sole change shape and lose and regain contact with the surface, with the “ripple” travelling at near supersonic speeds.
The pitch of the squeak even matches the rate of the “bursts”, which is determined by the stiffness and thickness of the shoe sole.
The authors also found that if a soft surface is smooth, the pulses are irregular and produce no sharp sounds, whereas ridged surfaces – like the grip patterns on sports shoes – produce consistent pulse frequencies, resulting in a high-pitched squeak.
In another twist, lab experiments showed that in some instances, the slip pulses are triggered by triboelectric discharges – miniature lightning bolts caused by the friction of the rubber.
Indeed, the physics of these pulses share similar features with fracture fronts in plate tectonics, and so a better understanding the dynamicsthat occur between two surfaces may offer insights into friction across a range of systems.
“These results bridge two fields that are traditionally disconnected: the tribology of soft materials and the dynamics of earthquakes,” notes Shmuel Rubinstein from Hebrew University. “Soft friction is usually considered slow, yet we show that the squeak of a sneaker can propagate as fast as, or even faster than, the rupture of a geological fault, and that their physics is strikingly similar.”
An international team of researchers has shown that superconductivity can be modified by coupling a superconductor to a dark electromagnetic cavity. The research opens the door to the control of a material’s properties by modifying its electromagnetic environment.
Electronic structure defines many material properties – and this means that some properties can be changed by applying electromagnetic fields. The destruction of superconductivity by a magnetic field and the use of electric fields to control currents in semiconductors are two familiar examples.
There is growing interest in how electronic properties could be controlled by placing a material in a dark electromagnetic cavity that resonates with an electronic transition in that material. In this scenario, an external field is not applied to the material. Rather, interactions occur via quantum vacuum fluctuations within the cavity.
Holy Grail
“The Holy Grail of cavity materials research is to alter the properties of complex materials by engineering the electromagnetic environment,” explains the team – which includes Itai Keren, Tatiana Webb and Dmitri Basov at Columbia University in the US.
They created an optical cavity from a small slab of hexagonal boron nitride. This was interfaced with a slab of κ-ET, which is an organic low-temperature superconductor. The cavity was designed to resonate with an infrared transition in κ-ET involving the vibrational stretching of carbon–carbon bonds.
Hexagonal boron nitride was chosen because it is a hyperbolic van der Waals material. Van der Waals materials are stacks of atomically-thin layers. Atoms are strongly bound within each layer, but the layers are only weakly bound to each other by the van der Waals force. The gaps between layers can act as waveguides, confining light that bounces back and forth within the slab. As a result the slab behaves like an optical cavity with an isofrequency surface that is a hyperboloid in momentum space. Such a cavity supports a large number of modes and vacuum fluctuations, which enhances interactions with the superconductor.
Superfluid suppression
The researchers found that the presence of the cavity caused a strong suppression of superfluid density in κ-ET (a superconductor can be thought of as a superfluid of charged particles). The team mapped the superfluid density using magnetic force microscopy. This involved placing a tiny magnetic tip near to the surface of the superconductor. The magnetic field of the tip cannot penetrate into the superconductor (the Meissner effect) and this results in a force on the tip that is related to the superfluid density. They found that the density dropped by as much as 50% near the cavity interface.
The team also investigated the optical properties of the cavity using scattering-type scanning near-field optical microscope (s-SNOM). This involves firing tightly-focused laser light at an atomic force microscope (AFM) tip that is tapping on the surface of the cavity. The scattered light is processed to reveal the near-field component of light from just the region of the cavity below the tip .
The tapping tip creates phonon polaritons in the cavity, which are particle-like excitations that couple lattice vibrations to light. Analysing the near-field light across the cavity confirmed that the carbon stretching mode of κ-ET is coupled to the cavity. Calculations done by the team suggest that cavity coupling reduces the amplitude of the stretching mode vibrations.
Physicists know that superconductivity can arise from interactions between electrons and phonons (lattice vibrations), So, it is possible that the reduction in superfluid density is related to the suppression of stretching-mode vibrations. This, however, is not certain because κ-ET is an unconventional superconductor, which means that physicists do not understand the mechanism that causes its superconductivity. Further experiments could therefore shed light on the mysteries of unconventional superconductors.
“We are confident that our experiments will prompt further theoretical pursuits,” the team tells Physics World. The researchers also believe that practical applications could be possible. “Our work shows a new path towards the manipulation of superconducting properties.”
On 26 April 2026, it will be 40 years since the explosion at Unit 4 of the Chernobyl Nuclear Power Plant – the worst nuclear accident the world has known. In the early hours of 26 April 1986, a badly designed reactor, operated under intense pressure during a safety test, ran out of control. A powerful explosion and prolonged fire followed, releasing radioactive material across Ukraine, Belarus, Russia, with smaller quantities spewing across Europe.
In this episode of Physics World Stories, host Andrew Glester speaks with Jim Smith, an environmental physicist at the University of Portsmouth. Smith began his academic life studying astrophysics, but always had an interest in environmental issues. His PhD in applied mathematics at Liverpool focused on modelling how radioactive material from Chernobyl was transported through the atmosphere and deposited as far away as the Lake District in north-western England.
Smith recounts his visits to the abandoned Chernobyl plant and the 1000-square-mile exclusion zone, now home to roaming wolves and other thriving wildlife. He wants a rational debate about the relative risks, arguing that the accident’s social and economic consequences have significantly outweighed the long-term impacts of radiation itself.
The discussion ranges from the politics of nuclear energy and the hierarchical culture of the Soviet system, to lessons later applied during the Fukushima accident. Smith makes the case for nuclear power as a vital complement to renewables.
He also shares the story behind the Chernobyl Spirit Company – a social enterprise he has launched with Ukrainian colleagues, producing safe, high-quality spirits to support Ukrainian communities. Listen to find out whether Andrew Glester dared to try one.
Later this year, CERN’s Large Hadron Collider (LHC) and its huge experiments will shutdown for the High Luminosity upgrade. When complete in 2030, the particle-collision rate in the LHC will be increased by a factor of 10 and the experiments will be upgraded so that they can better capture and analyse the results of these collisions. This will allow physicists to study particle interactions at unprecedented precision and could even reveal new physics beyond the Standard Model.
Earlier this year, however, the UK government announced that it will no longer fund the upgrade of the LHCb experiment on the LHC, which is run by a collaboration of more than 1700 physicists worldwide. The UK had promised to contribute about £50 million to the upgrade – which is a significant chunk of the overall cost.
In this episode of the Physics World Weekly podcast I am in conversation with the particle physicist Tim Gershon, who is based at the UK’s University of Warwick. Gershon is spokesperson-elect for the LHCb collaboration and is playing a leading role in the upgrade.
Gershon explains that UK participation and leadership has been crucial for the success of LHCb and cautions that the future of the experiment and the future of UK particle physics have been imperilled by the funding cut.
We also chat about recent discoveries made by LHCb and look forward to what new physics the experiment could find after the upgrade.
Quantum computers could solve problems that are out of reach for today’s classical machines. However, the quantum states they rely on are prone to decohering – that is, losing their quantum information due to local noise. One possible way around this is to use quantum bits (qubits) constructed from quasiparticle states known as Majorana zero modes (MZMs) that are protected from this noise. But there’s a catch. To perform computations, you need to be able to measure, or read out, the states of your qubits. How do you do that in a system that is inherently protected from its environment?
Scientists at QuTech in the Netherlands, together with researchers from the Madrid Institute of Materials Science (ICMM) in Spain, say they may have found an answer. By measuring a property known as quantum capacitance, they report that they have read out the parity of their MZM system, backing up an earlier readout demonstration from a team at Microsoft Quantum Hardware on a different Majorana platform.
Measuring parity
The QuTech/ICMM researchers generated their MZMs across two quantum dots – semiconductor structures that can confine electrons – connected by a superconducting nanowire. Electrons can transfer, or tunnel, between the quantum dots through this wire. Majorana-based qubits store their quantum information across these separated MZMs, with both elements in the pair required to encode a single “parity” bit. A pair of parity bits (combining four MZMs in total) forms a qubit.
A parity bit has two possible states. When the two quantum dots are in a superposition of both having one electron and both having none, the system is said to have even parity (a “0”). When the system is instead in superposition of only one of the quantum dots having an electron, the parity is said to be odd (a “1”). Importantly, these even and odd parity states have the same average value of electric charge, meaning that a charge sensor cannot tell them apart.
The key to measuring parity lies in the electrons’ behaviour. In the even-parity state, an even number of electrons can pair up and enter the superconductor together as a Cooper pair. In the odd-parity state, however, the lone electron lacks a partner and cannot flow through the wire in the same way. By measuring the charge flowing into the superconductor, the team was therefore able to determine the parity state. The researchers also determined that the lifetimes of these states were in the millisecond range, which they say is promising for quantum computations.
Competing platforms
According to Nick van Loo, a quantum engineer at QuTech and the first author of a Nature paper on the work, similar chains of quantum dots (known as Kitaev chains) are a promising platform for realizing Majorana modes because each element in the chain can be controlled and tuned. This control, he adds, makes results easier to reproduce, helping to overcome some of the interpretation challenges that have affected Majorana results over the past decade.
Van Loo also stresses that his team uses a different architecture from the Microsoft Quantum Hardware team to create its Majorana modes – one that he says allows for better tuneability as well as easier and more scalable readout. He adds that this architecture also allows an independent charge sensor to be used to confirm the MZM’s charge neutrality.
In response, Chetan Nayak, a technical fellow at Microsoft Quantum Hardware, says it is important that the QuTech/ICMM team independently measured a millisecond time scale for parity fluctuations. However, he notes that the team did not extend this parity lifetime and adds that the so-called “poor man’s Majoranas” used in this research do not constitute a scalable platform for topological qubits, as they lack topological protection.
Seeking full protection
Van Loo acknowledges that the team’s two-site Kitaev chain is not topologically protected. However, he says the degree of protection is expected to improve exponentially as more sites are added. In the near term, he and his colleagues hope to operate their qubit by inducing rotations through coupling pairs of Majorana modes. Once these hurdles are overcome, he tells Physics World that “one major milestone will still remain: demonstrating braiding of Majorana modes to establish their non-Abelian exchange statistics”.
Jay Deep Sau, a physicist at the University of Maryland, US, who was not involved in either the QuTech/ICMM or the Microsoft Quantum Hardware research, describes this as the first measurement of fermion parity in the smallest quantum dot chain platform for creating MZMs. Compared to the Microsoft result, Sau agrees that the quantum dot chain is more controlled. However, he is sceptical that this control will apply to larger chains, casting doubt on whether this is truly a scalable way of realizing MZMs. The significance of these results, he adds, will only be apparent if the quantum dot chain approach can demonstrate a coherent qubit before its semiconductor nanowire counterpart.
Researchers in China have distributed device-independent quantum cryptographic keys over city-scale distances for the first time – a significant improvement compared to the previous record of a few hundred metres. Led by Jian-Wei Pan of the University of Science and Technology of China (USTC) of the Chinese Academy of Sciences (CAS), the researchers say the achievement brings the world a step closer to a completely quantum-secure Internet.
Many of us use Internet encryption almost daily, for example when transferring sensitive information such as bank details. Today’s encryption techniques use keys based on mathematical algorithms, and classical supercomputers cannot crack them in any practical amount of time. Powerful quantum computers could change this, however, which has driven researchers to explore potential alternatives.
One such alternative, known as quantum key distribution (QKD), encrypts information by exploiting the quantum properties of photons. The appeal of this approach is that when quantum-entangled photons transmit a key between two parties, any attempted hack by a third party will be easy to detect because their intervention will disturb the entanglement.
While the basic form of QKD enables information to be transmitted securely, it does have some weak points. One of them is that a malicious third party could steal the key by hacking the devices the sender and/or receiver is using.
A more advanced version of QKD is device-independent QKD (DI-QKD). As its name suggests, this version does not depend on the state of a device. Instead, it derives its security key directly from fundamental quantum phenomena – namely, the violation of conditions known as Bell’s inequalities. Establishing this violation ensures that a third party has not interfered with the process employed to generate the secure key.
The main drawback of DI-QKD is that it is extremely technically demanding, requiring high-quality entanglement and an efficient means of detecting it. “Until now, this has only been possible over short distances – 700 m at best – and in laboratory-based proof-of-principle experiments,” says Pan.
High-fidelity entanglement over 11 km of fibre
In the latest work, Pan and colleagues constructed two quantum nodes consisting of single trapped atoms. Each node was equipped with four high-numerical-aperture lenses to efficiently collect single photons emitted by the atoms. These photons have a wavelength of 780 nm, which is not optimal for transmission through optical fibres. The team therefore used a process known as quantum frequency conversion to shift the emitted photons to a longer wavelength of 1315 nm, which is less prone to optical loss in fibres.
By interfering and detecting a single photon, the team was able to generate what’s known as heralded entanglement between the two quantum nodes – something Pan describes as “an essential resource” for DI-QKD. While significant progress has been made in extending the entangling distance for qubits of this type, Pan notes that these advances have been hampered by low fidelities and low entangling rates.
To address this, Pan and his colleagues employed a single-photon-based entangling scheme that boosts remote entangling probability by more than two orders of magnitude. They also placed their atoms in highly excited Rydberg states to generate single photons with high purity and low noise. “It is these innovations that allow us to achieve high-fidelity and high-rate entanglement over a long distance,” Pan explains.
Using this setup, the researchers explored the feasibility of performing DI-QKD between two entangled atoms linked by optical fibres up to 100 km in length. In this study, which is detailed in Science, they demonstrated practical DI-QKD under finite-key security over 11 km of fibre.
Metropolitan-scale quantum key distribution
Based on the technologies they developed, Pan thinks it could now be possible to implement DI-QKD over metropolitan scales with existing optical fibres. Such a system could provide encrypted communication with the highest level of physical security, but Pan notes that it could also have other applications. For example, high-fidelity entanglement could also serve as a fundamental building block for constructing quantum repeaters and scaling up quantum networks.
Carlos Sabín, a physicist at the Autonomous University of Madrid (UAM), Spain, who was not involved in the study, says that while the work is an important step, there is still a long way to go before we are able to perform completely secure and error-free quantum key distribution on an inter-city scale. “This is because quantum entanglement is an inherently fragile property,” Sabín explains. “As light travels through the fibre, small losses accumulate and the entanglement generated is of poorer quality, which translates into higher error rates in the cryptographic keys generated. Indeed, the results of the experiment show that errors in the key range from 3% when the distance is 11 km to more than 7% for 100 km.”
Pan and colleagues now plan to add more atoms to each node and to use techniques like tweezer arrays to further enhance both the entangling rate and the secure key rate over longer distances. “We are aiming for 1000 km, over which we hope to incorporate quantum repeaters,” Pan tells Physics World. “By using processes like ‘entanglement swapping’ to connect a series of such two-node entanglement, we anticipate that we will be able maintain a similar entangling rate for much longer distances.”
Todd McNutt is a radiation oncology physicist at Johns Hopkins University in the US and the co-founder of Oncospace, where he led the development of an artificial intelligence (AI)-powered tool that simultaneously accelerates radiation planning and elevates plan quality and consistency. The software, now rebranded as Plan AI and available from US manufacturer Sun Nuclear, draws upon data from thousands of previous radiotherapy treatments to predict the lowest possible dose to healthy tissues for each new patient. Treatment planners then use this information to define goals that streamline and automate the creation of a best achievable plan.
Physics World’s Tami Freeman spoke with McNutt about the evolution of Oncospace and the benefits that Plan AI brings to radiotherapy patients and cancer treatment centres.
Can you describe how the Oncospace project began?
Back in 2007, several groups were discussing how we could better use clinical data for discovery and knowledge generation. I had several meetings with folks at Johns Hopkins, including Alex Szalay who helped develop the Sloan Digital Sky Survey. He built a large database of galaxies and stars and it became a huge research platform for both amateur and professional astronomers.
From that discussion, and other initiatives, we looked at moving towards structured data collection for patients in the clinical environment. By marrying these data with radiation treatment plans we could study how dose distributions across the anatomy affect patient outcomes. And we took that opportunity to build a database for radiotherapy.
What inspired the transition from academic research to founding the company Oncospace Inc in 2019?
After populating the database with data from many patients, we could examine which anatomic features impact our ability to generate a plan that minimizes radiation dose to normal tissues while treating target volumes as best as possible. We came up with a feature set that characterized the relationships between normal anatomy and targets, as well as target complexity.
This early work allowed us to predict expected doses from these shape-relationship features, and it worked well. At that point, we knew we could tap into this database and generate a prediction that could help create treatment plans for new patients. We thought of this as personalized medicine: for the first time, we could see the level of treatment plan quality that we could achieve for a specific patient.
I thought that this was useful commercially and that we should get it out to other clinics. Praveen Sinha, who I’d known from my previous work at Philips and now leads Sun Nuclear’s software business line, asked if I wanted to create a startup. The timing was right for both of us and I had a team here ready to go, so we went ahead and did it. With his knowledge of startups and my knowledge of what we wanted to achieve, we had perfect timing and a perfect group to work with.
Plan AI enables both predictive planning and peer review, how do these functions work?
The idea behind predictive planning is that, for a given patient, I can predict the expected dose that I should be able to achieve for them.
Plan AI software Comparing dose–volume histogram prediction bands with clinical goals (arrows) provides users with valuable feedback on what can be achieved before the planning process begins. The screen shows the prediction sent to the treatment planning system.Clinical plan The screen shows a review of the results that the treatment planning system achieved, with dose–volume histograms shown by the solid lines.
Treatment planning involves specifying dosimetric objectives to the planning system and asking it to optimize radiation delivery to meet these. But nobody really knows what the right objectives even are – it is just a trial-and-error process. Plan AI’s prediction provides a rational set of objectives for plan optimization, allowing the planning system’s algorithm to move towards a good solution and making treatment planning an easier problem to solve.
Peer review involves a peer physician looking at every treatment plan to evaluate it for quality and safety. But again, people don’t really know the level of quality you can generate, it depends on the patient’s anatomy. Providing a predicted dose with clinical dose goals enables a rapid review to see whether it is a high-quality plan or not.
In the past we looked at simple things like whether a contour is missing slices or contains discontinuities and Plan AI checks for this, but you can do far more with AI. For example, you could look at all the contoured rectums in the system and predict if your contour goes too far into the sigmoid colon, then it may be mis-contoured. We have research software that can flag such potential anomalies so they don’t get overlooked.
The Plan AI models are developed using Oncospace’s database of previous treatments; can you describe this data lake?
When we first started, we developed a large SQL database containing all the shape-relationship features and dosimetry features. The SQL language is ideal for being able to query and sift through the data, but when the company was formed, we recognized that there was some age to that technology.
So for the Plan AI data lake, we extracted all the different shape-relationship and shape-complexity features and put them into a Parquet database in the cloud. This made the data lake much more amenable to applying machine learning algorithms to it. The SQL data lake at Johns Hopkins is maintained separately and primarily used to investigate toxicity predictions and spatial dose patterns. But for Plan AI, the models are fixed and streamlined for the specific task of dose prediction.
What does the model training process entail?
One of the first tasks was to curate the data, using the AAPM’s standardized structure-naming model. Our data scientist Julie Shade wrote some tools for automatic name mapping and target identification; that helped us process much larger amounts of data for the model.
Once we had all the shape-relationship and shape-complexity features and all the doses, we trained the models by anatomical region. We have FDA-approved models for the male and female pelvis, thorax, abdomen and head-and-neck. For each of these, we predict the doses for every organ-at-risk. Then we used a five-fold validation model to make sure that the predictions were good on an internal data set.
We also performed external validation at institutions including Johns Hopkins and Montefiore hospitals. We created predicted plans from recent treatment plans that had been evaluated by physicians. For almost all cases, both plan quality and plan efficiency were improved with Plan AI.
One aspect of this training is that whenever we drive optimization via predictive planning we want to push towards the best achievable dose. Regular machine learning predicts an expected, or average, dose across all patients. But you never want to drive a treatment plan towards the average dose, because then every plan you generate will be happy being average. Our model predicts both the average and the best achievable dose, and drives plan optimization towards the best achievable.
When implementing new technology in the clinic, it’s important to fit into the existing treatment workflow. How clinic-ready are these AI tools?
Radiation therapy is protocol-driven: we know what technique we’re going to use to treat and what our clinical dose goals are for different structures. What we don’t know is the patient-specific part of that. So for each anatomical region, we built models out of a wide range of treatment protocols, with many different types of patients, to ensure that the same prediction model works for any protocol. This means a user can use any protocol for treatment and the predictions will work, they don’t have to retrain anything. It’s ready to go out of the box, there’s a library of protocols to start with, and you can change protocols as you need for your own clinic.
The other part of being clinic-ready is aligning with the way that planning is currently performed, which is using dose–volume histograms. Treatment plans are optimized by manipulating these dose objectives, and that’s exactly what we predict. So users aren’t changing the whole paradigm of how planners operate. They still use their treatment planning system (TPS) – we just put the objectives in there. Basically, a TPS script sends the patient’s CT and contours to the cloud, where Plan AI makes the predictions. The TPS then pulls back in the objectives built from the models, based on this specific patient’s anatomy. The TPS runs the optimization and, as a last step, can send the plan back to Plan AI to check that it fits within the best achievable predictions.
Did you encounter any challenges bringing AI into a clinical setting?
Interestingly, the challenges aren’t technical, they are more human related. One of the more systemic challenges is data security when using medical data for training. A nice thing about our system is that the features we generate from treatment plans are just mathematical shape-relationship features and don’t involve a lot of identifiable information.
AI has been used in radiation therapy for image contouring and auto-segmentation, and early efforts were not so good. So, there’s always a good, healthy scepticism. But once you show people that it works and works well, this can be overcome. I have seen some people worried about job security and AI taking over. We are medical professionals designing a treatment plan to care for a patient and there’s a lot of pride and art in that – if you automate that, it takes away some of this pride and art.
I tell people that if we automate the easier things, then they can spend their quality time on the more difficult and challenging cases, because that’s where their talent might be needed more.
Do you have any advice for clinics looking to adopt AI-driven planning?
Introduce it as an assistant, not as a solution. You want people that already know what they’re doing to be able to use their knowledge more efficiently. We want to make their jobs easier and show them that it also improves quality.
With dosimetrists, for example, they create a plan and work hard getting the dose down – and then the physician looks at it and suggests that they can do better. Predictive planning gives them confidence that they are right and takes the uncertainty out of the physician review process. And once you’ve gained that level of confidence, you can start using it for adaptive planning or other technologies.
Where do you see predictive modelling and AI in oncology in five years from now?
Right now, there’s been a lot of data collected, but we want that data to advance and learn. Having multiple centres adding to this pool of knowledge and being able to continually update those models from new, broader data sets could be of huge value.
In terms of patient outcomes, we’ve done a lot of the work looking at how the spatial pattern of dose impacts toxicity and outcomes. This is part of the research being performed at Johns Hopkins and still in discovery mode. But down the road, some of these predictions of normal tissue outcomes could be fed into the planning process to help reduce toxicity at the patient level.
Finally, what’s been the most rewarding part of this journey for you?
During my prior experience building treatment planning systems, the biggest problem was always that nobody knew what the objective was. Nobody knew how to tell the system: “this is the dose I expect to receive, now optimize to get it for me”, because you didn’t know what you could do. For any given patient, you could ask for too much or too little. Now, for the first time, I argue that we actually know what our objective is in our treatment planning.
This levels the playing field between different environments, different countries, or even different dosimetrists with different levels of experience. The Plan AI tool brings all this to a consistent state and enables high quality, efficient planning everywhere. We can provide this predictive planning tool to clinics around the world. Now we just have to get everybody using it.
In his opening remarks to the 4th International Symposium on the History of Particle Physics, Chris Llewellyn Smith – who was a director-general of CERN in the 1990s – suggested participants should speak about “what’s not written in the journals”, including “mistakes, dead-ends and problems with getting funding”. Doing so, he said, would “provide insight into the way science really progresses”.
The symposium was not your usual science conference. Held last November at CERN, it took place inside the lab’s 400-seat main auditorium, which has been the venue for many historic announcements, including the discovery of the Higgs boson. Its brown-beige walls are covered with lively designs by the Finnish artist Ilona Rista, suggesting to me the aftermath of a collision of high-energy bar codes.
The 1980s and 1990s saw the construction and operation of various important accelerators and detectors.
The focus of the meeting was the development of particle physics in the 1980s and 1990s – a period that saw the construction and operation of various important accelerators and detectors. At CERN, these included the UA1 and UA2 experiments at the Super Proton Synchrotron, where the W and Z bosons were discovered. Later, there was the Large Electron-Positron Collider (LEP), which came online in 1989, and the Large Hadron Collider (LHC), approved five years later.
Delegates also heard about the opening of various accelerators in the US during those two decades, including two at the Stanford Linear Accelerator Center – the Positron-Electron Project in 1980 and the Stanford Linear Collider in 1989. Most famous of all was the start-up of the Tevatron at Fermilab in 1983. Over at Dubna in the former Soviet Union, meanwhile, scientists built the Nuclotron, a superconducting synchrotron, which opened in 1992.
Conference speakers covered unfinished machines of the era as well. The US cancelled two proton–proton facilities – ISABELLE in 1983 and the Superconducting Super Collider (SSC) a decade later. The Soviet Union, meanwhile, abandoned the multi-TeV proton–proton collider UNK a few years later, though news has recently emerged that Russia might revive the project.
Several speakers recounted the discovery of the W and Z particles at CERN in 1983 and the discovery of the top quark at Fermilab in 1995. Others addressed the strange fact that fewer neutrinos from the Sun had been detected than theory suggested. The “solar-neutrino problem”, as it was known, was finally resolved by Takaaki Kajita’s discovery of neutrino oscillation in 1998, for which he shared the 2015 Nobel Prize for Physics with Art McDonald.
The conference also addressed unsuccessful searches for proton decay, axions, magnetic monopoles, the Higgs boson, supersymmetry particles and other targets. Other speakers described projects with highly positive outcomes, such as the advent of particle cosmology, or what some have jokingly dubbed “the heavenly lab”. The development of string theory, grand unified theories and perturbative quantum chromodynamics was tackled too.
In an exchange in the question-and-answer session after one talk, the Greek physicist Kostas Gavroglu referred to many of such quests as “failures”. That remark prompted the Australian-born US theoretical physicist Helen Quinn to say she preferred the term “falling forward”; such failures, she said, were instances of “I tried this, and it didn’t work so I tried that”.
In relating his work on detecting gravitational waves, the US Nobel-prize-winning physicist Barry Barish said he felt his charge was not to celebrate the importance of his discoveries nor the ingenuity of the route he took. Instead, Barish explained, his job was to answer the much more informal question: “What made me do what?”.
His point was illustrated by the US theorist Alan Guth, who described the very human and serendipitous path he took to working on cosmic inflation – the super-fast expansion of the universe just after the Big Bang. When he started, Guth said, “all the ingredients were already invented”. But the startling idea of inflation hinged on accidental meetings, chance conversations, unexpected visits, a restricted word count for Physical Review Letters, competitions, insecurities and “spectacular realizations” coalescing.
Wider world
Another theme that arose in the conference was that science does not unfold inside its own bubble but can have extensive and immediate impacts on the world around it. Two speakers, for instance, recounted the invention of the World Wide Web at CERN in the late 1980s. It’s fair to say that no other discovery by a single individual – Tim Berners-Lee – has so radically and quickly transformed the world.
The growing role of international politics in promoting and protecting projects was mentioned too, with various speakers explaining how high-level political negotiations enabled physicists to work at institutions and experiments in other nations. The Polish physicist Agnieszka Zalewska, for example, described her country’s path to membership in CERN, while Russian-born US physicist Vladimir Shiltsev spoke about the “diaspora” of Russian particle physicists after the fall of the Soviet Union in 1991.
As a result of the Superconducting Super Colllider’s controversial closure, the centre of gravity of high-energy physics shifted to Europe.
Sometimes politics created destructive interference. The US physicist, historian and author Michael Riordan described how the US’s determination to “go it alone” to outcompete Europe in high-energy physics was a major factor in bringing about the opposite: the termination of the SSC in 1993. As a result of that project’s controversial closure, the centre of gravity of high-energy physics shifted to Europe.
Indeed, contemporary politics occasionally hit the conference itself in incongruous and ironic ways. Two US physicists, for example, were denied permission to attend because budgets had been cut and travel restrictions increased. In the end, one took personal time off and paid his own way, leaving his affiliation off the programme.
Before the conference, some people complained that conference organizers hadn’t paid enough attention to physicists who’d worked in the Soviet Union but were from occupied republics. Several speakers addressed this shortcoming by mentioning people like Gersh Budker (1918–1977). A Ukrainian-born physicist who worked and died in the Soviet Union, Budker was nominated for a Nobel Prize (1957) and even has had a street named after him at CERN. Unmentioned, though, was that Budker was Jewish and that his father was killed by Ukrainian nationalists in a pogrom.
On the final day of the conference, which just happened to be World Science Day for Peace and Development, CERN mounted a public screening of the 2025 documentary film The Peace Particle. Directed by Alex Kiehl, much of it was about CERN’s internationalism, with a poster for the film describing the lab as “Mankind’s biggest experiment…science for peace in a divided world”.
But in the Q&A afterwards some audience members criticized CERN for allegedly whitewashing Russia for its invasion of the Ukraine and Israel for genocide. Those onstage defended CERN on the grounds of its desire to promote internationalism.
The critical point
The keynote speaker of the conference was John Krige, a science historian from Georgia Tech who has worked on a three-volume history of CERN. Those who launched the lab, Krige reminded the audience, had radical “scientific, political and cultural aspirations” for the institution. Their dream was that CERN wouldn’t just revive European science and promote regional collaborative effects after the Second World War, but also potentially improve the global world order too.
Krige went on to quote one CERN founder, who’d said that international science facilities such as CERN would be “one of the best ways of saving Western civilization”. Recent events, however, have shown just how fragile those ambitions are. Alluding to CERN’s Future Circular Collider and other possible projects, Llewellyn Smith ended his closing remarks with a warning.
“The perennial hope that the next big high-energy project will be genuinely global,” he said, “seems to be receding over the horizon due to the polarization of world politics”.